-
Question 1
Incorrect
-
Question 2
Incorrect
-
When deciding on entry method for laparoscopy a patients build is important. Which of the following entry methods is inappropriately matched to the patient?
Your Answer: Varess needle entry into a patient (BMI 28)
Correct Answer: Varess needle entry in a very thin patient (BMI 16)
Explanation:In patients with normal BMI there is no preferential entry method. The Varess technique is not appropriate for morbidly obese or very thin patients for the reasons set out below: Morbid Obesity (BMI>40): Hasson technique or entry at Palmers point Reason: difficult penetration with Varess needle Very Thin Patients: Hasson technique or insertion at Palmers point Reason: higher risk of vascular injury
-
This question is part of the following fields:
- Clinical Management
-
-
Question 3
Incorrect
-
A 30 year old women who is 24 weeks pregnant attends EPU due to suprapubic pain. Ultrasound shows a viable foetus and also a fibroid with a cystic fluid filled centre. What is the likely diagnosis?
Your Answer: Cystic degeneration of fibroid
Correct Answer: Red degeneration of fibroid
Explanation:Red degeneration of fibroids is one of 4 methods of fibroid degeneration. Although uncommon outside pregnancy it is thought to be the most common form of fibroid degeneration during pregnancy and typically occurs in the 2nd trimester. It is thought to arise from the fibroid outgrowing its blood supply and haemorrhagic infarction occurs. Ultrasound will typically show a localised fluid collection (blood) within the fibroid.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 4
Correct
-
A 30 year old patient attends for non-invasive pre-natal screening for Down's syndrome. You advise her that the result will take the form of a risk score and higher risk results will be offered CVS or amniocentesis. What is the cut-off figure between low and high risk?
Your Answer: 1 in 150
Explanation:1 in 150 is the cut off. Where pre-natal screening shows a risk of 1 in 150 or greater invasive testing is typically offered.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 5
Incorrect
-
A patient is attending for medical abortion. She is 15 weeks gestation. She has no known drug allergies. Which of the following is the most appropriate regarding antibiotic prophylaxis?
Your Answer: Doxycycline 100mg twice daily for 7 days starting on day of abortion
Correct Answer: Stat Azithromycin 1g and metronidazole 800 mg orally at time of abortion
Explanation:If the patient has a negative Chlamydia screen then a stat dose of metronidazole monotherapy is appropriate. You do not know this patients Chlamydia status and therefore dual therapy with metronidazole + doxycycline or azithromycin is appropriate.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 6
Correct
-
You are asked to review a patient. They have attended for a scan at 13 weeks following a positive pregnancy test. The patient has had 2 previous pregnancies for which she opted for termination on both occasions. The scan shows a large irregular haemorrhagic mass that appears to be invading into the myometrium. What is the likely diagnosis?
Your Answer: Choriocarcinoma
Explanation:Choriocarcinoma may arise as a complication of gestation or as spontaneous germ cell tumours. As this scenario depicts that the women has previous abortion points to the fact that these may have been molar pregnancies. As choriocarcinoma can arise from a molar pregnancy it can be differentiated from it by the presence of invasion into the uterus and metastasis to the lungs primarily.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 7
Incorrect
-
A 34 week pregnant patient complains of itching over the past 6 weeks particularly to the hands and feet which is worse at night. You order some blood tests. Which of the following would you normally expect to increase in the 3rd trimester?
Your Answer: Calcium
Correct Answer: ALP
Explanation:Pruritus of pregnancy is a common disorder, which occurs in 1 in 300 pregnancies, and presents as excoriated papules on extensor limbs, abdomen
and shoulders. It is more common in women with a history of atopy. Prurigo usually starts at around 25–30 weeks of pregnancy and resolves after delivery,
with no effect on the mother or baby. Treatment is symptomatic with topical steroids and emollients. It occurs due to derangement in the LFTs. ALP can rise to up to 3 times the normal non-pregnant value in the 3rd trimester.
All of the other tests above typically decrease during pregnancy. -
This question is part of the following fields:
- Clinical Management
-
-
Question 8
Correct
-
Which one of the following has the most significant effect on slowing drug metabolism in pregnancy?
Your Answer: Progesterone effect on gastric motility
Explanation:Progesterone down regulates gastric motility meaning drugs are absorbed and metabolised more slowly, thus drugs are absorbed, metabolised and cleared more slowly. Most of the drugs are transported after binding to the albumin.
Lower albumin levels mean a greater unbound drug fraction but as this may be thought to increase drug concentrations it actually leaves more available for hepatic clearance or renal excretion so overall drug concentrations are unchanged and metabolism increased.
Increase in hepatic flow will increase the metabolism of the drug as the drug will be transported faster.
Increased renal blood flow will result in the faster clearance of the drug from the body. -
This question is part of the following fields:
- Clinical Management
-
-
Question 9
Incorrect
-
In a patient who undergoes a medical abortion at 10 weeks gestation, what advice would you give regarding Rhesus Anti-D Immunoglobulin?
Your Answer: Not required
Correct Answer: All RhD-negative women who are not alloimmunized should receive Anti-D IgG
Explanation:The Rhesus status of a mother is important in pregnancy and abortion. The exposure of an Rh-negative mother to Rh antigens from a positive foetus, will influence the development of anti-Rh antibodies. This may cause problems in subsequent pregnancies leading to haemolysis in the newborn. Rh Anti RhD- globulin is therefore given to non-sensitised Rh-negative mothers to prevent the formation of anti-Rh antibodies within 72 hours following abortion. Anti RhD globulin is not useful for already sensitized, or RhD positive mothers.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 10
Incorrect
-
A 36 year old patient is diagnosed with cervical cancer and staging investigations show there is parametrial involvement but it is confined within the pelvic wall and does not involve the lower 1/3 vagina. There is no evidence of hydronephrosis. What FIGO stage is this?
Your Answer: 2A
Correct Answer: 2B
Explanation:It is stage 2B. Stage I: is strictly confined to the cervix; extension to the uterine corpus should be disregarded. The diagnosis of both Stages IA1 and IA2 should be based on microscopic examination of removed tissue, preferably a cone, which must include the entire lesion.
2010 FIGO classification of cervical carcinoma:
Stage IA: Invasive cancer identified only microscopically. Invasion is limited to measured stromal invasion with a maximum depth of 5 mm and no wider than 7 mm.
Stage IA1: Measured invasion of the stroma no greater than 3 mm in depth and no wider than 7 mm diameter.
Stage IA2: Measured invasion of stroma greater than 3 mm but no greater than 5 mm in depth and no wider than 7 mm in diameter.Stage IB: Clinical lesions confined to the cervix or preclinical lesions greater than Stage IA. All gross lesions even with superficial invasion are Stage IB cancers.
Stage IB1: Clinical lesions no greater than 4 cm in size.
Stage IB2: Clinical lesions greater than 4 cm in size.Stage II: carcinoma that extends beyond the cervix, but does not extend into the pelvic wall. The carcinoma involves the vagina, but not as far as the lower third.
Stage IIA: No obvious parametrial involvement. Involvement of up to the upper two-thirds of the vagina.
Stage IIB: Obvious parametrial involvement, but not into the pelvic sidewall.Stage III: carcinoma that has extended into the pelvic sidewall. On rectal examination, there is no cancer-free space between the tumour and the pelvic sidewall. The tumour involves the lower third of the vagina. All cases with hydronephrosis or a non-functioning kidney are Stage III cancers.
Stage IIIA: No extension into the pelvic sidewall but involvement of the lower third of the vagina.
Stage IIIB: Extension into the pelvic sidewall or hydronephrosis or non-functioning kidney.Stage IV: carcinoma that has extended beyond the true pelvis or has clinically involved the mucosa of the bladder and/or rectum.
Stage IVA: Spread of the tumour into adjacent pelvic organs.
Stage IVB: Spread to distant organs. -
This question is part of the following fields:
- Clinical Management
-
-
Question 11
Incorrect
-
What is the prevalence of antiphospholipid syndrome in patients with recurrent miscarriage?
Your Answer: 2.50%
Correct Answer: 15%
Explanation:Anti phospholipid syndrome is an autoimmune disorder in which abnormal antibodies are formed which increases the risk of blood clots to develop in vessels and leads to recurrent miscarriages to occurs. The changes of recurrent miscarriage in a previously known case of APL is 15%.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 12
Incorrect
-
Regarding pelvic inflammatory disease, which of the following is the tubal factor infertility rate?
Your Answer: 25%
Correct Answer: 12.50%
Explanation:Pelvic inflammatory disease (PID) is a known risk factor in causing tubal infertility due to its role in tubal damage. The tubal infertility rate after one episode of PID is thought to be about 12.5%. After two episodes the risk increases to 25%, and 50% after three episodes. The usual causative agents are chlamydia and gonorrhoea.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 13
Incorrect
-
A patient attends the maternity unit as her waters have broken but she hasn't had contractions. She is 39+6 weeks gestation. Speculum examination confirms prelabour rupture of membranes (PROM). According to NICE guidelines after what time period should induction be offered?
Your Answer: 12 hours
Correct Answer: 24 hours
Explanation:Induction of labour is appropriate approximately 24 hours after rupture of the membranes.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 14
Correct
-
A patient is being discharged following a termination of pregnancy at 14 weeks. She had been taking Microgynon in the past but stopped taking this 6 months prior to falling pregnant as she wasn't in a serious relationship.
Your Answer: Start immediately
Explanation:Combined oral contraceptive pills (COCPs) can be started immediately following abortion or miscarriage. Note following childbirth COCPs should not be restarted for 3 weeks (assuming the patient is not breastfeeding).
-
This question is part of the following fields:
- Clinical Management
-
-
Question 15
Correct
-
You are attending the labour of a patient who has had a prolonged 1st stage of labour. You note the fetal head start to retract after being tightly applied to the vulva (turtle-neck sign). What is the next most appropriate management step?
Your Answer: McRoberts' manoeuvre
Explanation:Signs of shoulder dystocia:
– Difficulty with delivery of the face and chin
– The head remaining tightly applied to the vulva or even retracting (turtle-neck sign)
– Failure of restitution of the fetal head
– Failure of the shoulders to descend
Upon identifying shoulder dystocia additional help should be called and McRoberts manoeuvre (flexion and abduction of the maternal hips, positioning the maternal thighs on her abdomen) should be performed first. Fundal pressure is associated with uterine rupture and should not be used. -
This question is part of the following fields:
- Clinical Management
-
-
Question 16
Incorrect
-
The amniotic fluid volume peaks at around 900ml. At what gestation does the amniotic fluid reach its maximum volume?
Your Answer: 32 weeks
Correct Answer: 35 weeks
Explanation:The amniotic fluid volume increases up to week 35 of gestation and then decreases from then to term.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 17
Incorrect
-
What is the most common Type II congenital thrombophilia?
Your Answer: Protein C deficiency
Correct Answer: Factor V Leiden mutation
Explanation:Factor V Leiden is the most common congenital thrombophilia. Named after the Dutch city Leiden where it was first discovered. Protein C and S deficiencies are type 1 (Not type 2) thrombophilias Antiphospholipid syndrome is an acquired (NOT congenital) thrombophilia
-
This question is part of the following fields:
- Clinical Management
-
-
Question 18
Incorrect
-
A patient asks you in clinic when she can start trying to conceive again. She has just completed chemotherapy for gestational trophoblastic disease (GTD)?
Your Answer: 6 weeks from completion of treatment
Correct Answer: 1 year from completion of treatment
Explanation:According to the RCOG greentop guidelines, a women who have underdone chemotherapy for GTD are advised not to conceive for 1 years after completion of the chemotherapy.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 19
Incorrect
-
Regarding the diagnosis of Gestational Diabetes which of the following tests is recommended by the WHO for diagnosis?
Your Answer: HBA1C
Correct Answer: 75g OGTT with 2 hour glucose
Explanation:Gestational diabetes (GDM) occurs in 2–9 per cent of all pregnancies. Screening for diabetes in pregnancy can be justify ed to diagnose previously unrecognized cases of pre-existing diabetes and to identify a group of women who are at risk of developing NIDDM later in life. No single screening test has been shown to be perfect in terms of high sensitivity and specific city for gestational diabetes. Urinary glucose is unreliable, and most screening tests now rely on blood glucose estimation, with an oral 75g glucose tolerance test commonly used. The aim of glucose control is to keep fasting levels between 3.5 and 5.5 mmol/L and postprandial levels 7.1 mmol/L, with insulin treatment usually indicated outside these ranges.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 20
Correct
-
A 28 year old patient is treated for hydatidiform mole with methotrexate. What is the mechanism of action of methotrexate?
Your Answer: Inhibits dihydrofolate reductase
Explanation:Methotrexate is a folic acid antagonist. It inhibits dihydrofolate reductase (DHFR). DHFR catalyses the conversion of dihydrofolate to the active tetrahydrofolate which is required for DNA synthesis. It is either administered as a single intramuscular injection or multiple fixed doses.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 21
Incorrect
-
Which of the following dugs is a strong inducer of cytochrome P450?
Your Answer: Topiramate
Correct Answer: Phenytoin
Explanation:It is important to be aware of which ant-epileptics induce cytochrome P450. Of the above Topiramate and Phenytoin are moderate and strong inducers respectively.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 22
Incorrect
-
When is the earliest appropriate gestational age to perform amniocentesis?
Your Answer: 10+0 weeks
Correct Answer: 15+0 weeks
Explanation:The best time to perform amniocentesis is at the gestational age of 15 weeks or more. There is increased risk of abortion, respiratory problems and fetal talipes if amniocentesis is performed before the gestational age of 14 weeks.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 23
Correct
-
A 26 year old patient who is currently 24 weeks pregnant presents with vaginal discharge. Swabs show Chlamydia Trachomatis detected. Which of the following is the most appropriate treatment regime?
Your Answer: Erythromycin 500 mg twice a day for 14 days
Explanation:The following treatment regimes are recommended for the treatment of Chlamydia in Pregnancy: Erythromycin 500mg four times a day for 7 days or Erythromycin 500 mg twice a day for 14 days or Amoxicillin 500 mg three times a day for 7 days or Azithromycin 1 gm stat (only if no alternative, safety in pregnancy not fully assessed) The following treatment regimes are recommended for the treatment of Chlamydia in NON-PREGNANT patients: Doxycycline 100mg bd for 7 days OR Azithromycin 1gm orally in a single dose NOTE: Doxycycline and Ofloxacin are contraindicated in pregnancy
-
This question is part of the following fields:
- Clinical Management
-
-
Question 24
Correct
-
Which species of candida is the most common cause of genital candida infection in pregnancy?
Your Answer: Candida albicans
Explanation:Vulvovaginal candidiasis is the most common genital infection and it is caused by candida albicans in 80-92% of the cases. Other non albicans species include C.tropicalis, C.glabrata, C.krusei and C.parapsilosis. 20% of women of childbearing age are asymptotic colonisers of Candida species as part of their normal vaginal flora. This increases to 40% in pregnancy.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 25
Incorrect
-
A 28 year old primigravida carrying a twin pregnancy presents at 32 weeks gestation. She is lethargic, clinically jaundiced and complains of abdominal pain with frequent vomiting. A summary of her blood results are as follows: Elevated aspartate transaminase (AST) and alanine transaminase (ALT) levels · Decreased blood glucose levels · Elevated levels of blood ammonia. What is the likely diagnosis?
Your Answer: Hepatitis A
Correct Answer: Acute fatty liver of pregnancy
Explanation:This patients bloods and symptoms suggest she has hepatic impairment. Acute fatty liver of pregnancy typically presents after the 30th week. The usual symptoms in the mother are non-specific including nausea, vomiting, anorexia (or lack of desire to eat) and abdominal pain; excessive thirst may be the earliest symptom without overlap with otherwise considered normal pregnancy symptoms; however, jaundice and fever may occur in as many as 70% of patients.
Many laboratory abnormalities are seen in acute fatty liver of pregnancy. Liver enzymes are elevated, with the AST and ALT enzymes ranging from minimal elevation to 1000 IU/L, but usually staying in the 300-500 range. Bilirubin is almost universally elevated. Alkaline phosphatase is often elevated in pregnancy due to production from the placenta, but may be additionally elevated. Other abnormalities may include an elevated white blood cell count, hypoglycemia, elevated coagulation parameters, including the international normalized ratio, and decreased fibrinogen. There may be increases of ammonia, uric acid aswell.
Recent studies have shown that being a primigravida, multiple pregnancies, carrying a male fetus, other liver diseases during pregnancy, previous history of AFLP, and pre-eclampsia are the potential risk factors for AFLP
-
This question is part of the following fields:
- Clinical Management
-
-
Question 26
Incorrect
-
Which of the following contraceptives primary mode of action is inhibition of ovulation?
Your Answer: Norgeston®
Correct Answer: Cerazette®
Explanation:Traditional POP main mode of contraceptive action: thickening of cervical mucus Desogestrel-only POP main mode of contraceptive action is inhibition of ovulation Cerazette® is the only Desogestrel-only POP in the options above. Other desogestrel brands include: Aizea® Cerelle® Nacrez® The other POPs listed are considered traditional POPs and have the following compositions: Norgeston® – Levonorgestrel 30 mcg Micronor® & Noriday® – Norethisterone 350 mcg Femulen® – Ethynediol diacetate 500 mcg
-
This question is part of the following fields:
- Clinical Management
-
-
Question 27
Correct
-
Breast feeding stimulates the hypothalamus to produce which of the following hormones?
Your Answer: Oxytocin
Explanation:Breast feeding facilitates the production of Oxytocin by the hypothalamus which is stored and secreted by the posterior pituitary.
Ergometrine is an ergoline derivative that can be used to increase uterine tone.
Atosiban is an antagonist of Oxytocin receptors
ADH is another posterior pituitary hormone.
Prostaglandin E2 plays an important role in cervical ripening. -
This question is part of the following fields:
- Clinical Management
-
-
Question 28
Correct
-
A 24 year old who is 32 weeks pregnant presents with a rash to the abdomen. Looking at the picture below what is the diagnosis?
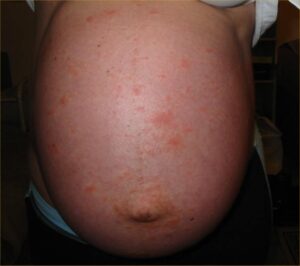
Your Answer: Polymorphic Eruption of Pregnancy
Explanation:This is Polymorphic Eruption of Pregnancy (PEP) also known as Pruritic Urticarial Papules and Plaques of Pregnancy (PUPPP). Papules and plaques form on the abdomen (commonly within striae). It is most common in women during their first pregnancy and typically occurs in the 3rd trimester.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 29
Incorrect
-
According to the RCOG Green-top guidelines on prevention and management of post-partum haemorrhage (PPH) which of the following statements is true?
Your Answer: Misoprostol is equally as effective as Oxytocin in PPH prevention
Correct Answer: For women delivering by caesarean section, Oxytocin 5 iu by slow IV injection should be used
Explanation:Misoprostol is not as effective as oxytocin but may be used if Oxytocin is not available e.g. home birth Recommended doses of Oxytocin For vaginal deliveries: 5 iu or 10 iu by intramuscular injection. For C-section: 5 iu by IV injection
-
This question is part of the following fields:
- Clinical Management
-
-
Question 30
Incorrect
00
Correct
00
Incorrect
00
:
00
:
0
00
Session Time
00
:
00
Average Question Time (
Mins)