-
Question 1
Correct
-
A 30-year-old female is being investigated for subfertility. At what day of her menstrual cycle should blood be collected for progesterone, if she has a regular 28-day menstrual cycle?
Your Answer: Day 21
Explanation:Maximum levels of progesterone are detected at day 21 of 28 days in the menstrual cycle, assuming that ovulation has occurred at day 14. A value of >30nmol/l indicates an ovulatory cycle.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 2
Correct
-
You are asked to see a 26 year old patient following her first visit to antenatal clinic. She is 9 weeks pregnant and bloods have shown her to be non-immune to Rubella. She is concerned about congenital rubella syndrome (CRS). What is the most appropriate advice to give?
Your Answer: Advise vaccination after birth regardless of breast feeding status
Explanation:Congenital rubella infection that occurs after 16 weeks gestation does not typically cause fetal abnormalities. This however plays no part in vaccination advice. Rubella vaccine is live and should not be given during pregnancy. The mother should be offered vaccination after giving birth. It is safe for the vaccine (typically given as combined MMR) to be administered if the mother is breastfeeding.
-
This question is part of the following fields:
- Microbiology
-
-
Question 3
Incorrect
-
The inguinal canal is reinforced posteriorly by which structure?
Your Answer: Internal oblique fibres
Correct Answer: Conjoint tendon
Explanation:The Inguinal Canal
– Anterior wall: formed by the external oblique aponeurosis throughout the length of the canal; its lateral part is reinforced by muscle fibres of the internal oblique.
– Posterior wall: formed by the transversalis fascia; its medial part is reinforced by pubic attachments of the internal oblique and transversus abdominis aponeuroses that frequently merge to variable extents into a common tendon—the inguinal falx (conjoint tendon)—and the reflected inguinal ligament.
– Roof: formed laterally by the transversalis fascia, centrally by musculo-aponeurotic arches of the internal oblique and transversus abdominis, and medially by the medial crus of the external oblique aponeurosis.
– Floor: formed laterally by the iliopubic tract, centrally by gutter formed by the infolded inguinal ligament, and medially by the lacunar ligament. -
This question is part of the following fields:
- Anatomy
-
-
Question 4
Incorrect
-
A 46 year old women with a BMI of 34 is seen in clinic following hysteroscopy and biopsy for irregular menstrual bleeding. Histology shows hyperplasia without atypia. Following a discussion the patient declines any treatment but agrees she will try and lose weight. What is the risk of progression to endometrial cancer over 20 years?
Your Answer: 20-30%
Correct Answer:
Explanation:The risk of developing endometrial carcinoma is less than 5% over 20 years if the endometrium shows hyperplasia without atypia.
There are 2 types of Endometrial Hyperplasia:
1. Hyperplasia without atypia*
2. Atypical hyperplasiaMajor Risk Factors:
Oestrogen (HRT)
Tamoxifen
PCOS
Obesity
Immunosuppression (transplant) -
This question is part of the following fields:
- Clinical Management
-
-
Question 5
Correct
-
A 32-year-old woman, at 37 weeks of gestation, presents to the emergency department due to sudden onset of severe abdominal pain with vaginal bleeding of approximately 1200 cc and cessation of contractions after 18 hours of active pushing at home. Her pregnancy has been uneventful until the event.
On examination, patient is conscious and pale, with a blood pressure of 70/45 mm of Hg and pulse rate of 115 bpm. Abdomen is found to be irregularly distended with shifting dullness and fluid thrill. Fetal heart sounds are not audible.
Which among of the following will most likely be her diagnosis?Your Answer: Uterine rupture
Explanation:The given case where the patient presents with sudden abdominal pain, cessation of uterine contraction and the urge to push along with vaginal bleeding is typical for uterine rupture. Examination shows a decreased or lost fetal heart rate, along with signs of fluid collection including fluid thrill and shifting dullness due to the entry of blood into the peritoneal cavity.
Other common manifestations of uterine rupture include:
– Loss of the station of the fetal presenting part
– Vaginal bleeding which is not be proportionate to the hemodynamic status
-Maternal tachycardia and hypotension ranging from subtle to severer shock
– Uterine tenderness
– Change in uterine shape and contour
– Easily palpable fetal parts
– No fetal presentation on vaginal examination
– Hematuria if the rupture extends to the bladder
Anterior lower transverse segment is the most common site of spontaneous uterine rupture.Placenta previa usually presents as painless vaginal bleeding, which rules it out as the diagnosis in given case.
Vaginal bleeding with a tender and tense uterus is the presentation in placental abruption, also contrary to uterine rupture, uterine contractions will continue in case of placental abruption.
Cervical laceration can be a possibility, but in such cases more amount of vaginal blood loss was expected in this patient with hemodynamic instability. Also symptoms like deformed uterus, abdominal distention and cessation of contractions are inconsistent with cervical laceration.
Excessive generation of thrombin and fibrin in the circulating blood results in Disseminated intravascular coagulation (DIC) which leads to increased platelets aggregation and consumption of coagulation factors resulting in consequent bleeding at one site and thromboembolism at another. Placental abruption and retained products of conception in the uterine cavity are the most common obstetric causes of DIC. The condition will not fit as diagnosis in this clinical scenario.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 6
Correct
-
A 26 year old primigravida woman attends A&E due to worsening vomiting. She is currently 10 weeks pregnant. For the past 4 weeks she has had morning sickness but for the last 4 days she has been unable to tolerate any oral fluids without vomiting and thinks she has lost weight. On questioning she has no significant past medical history prior to this pregnancy. She is currently taking the following medication:
Your Answer: Hyperemesis gravidarum
Explanation:This patient has severe nausea and vomiting with ketosis and evidence of dehydration (low BP and tachycardia) in the early part of pregnancy. There is no history of diabetes and the blood glucose doesn’t indicate hyperglycaemia. This is consistent with hyperemesis gravidarum (HG)
-
This question is part of the following fields:
- Clinical Management
-
-
Question 7
Correct
-
A 36-year-old obese woman presents to your office for advice regarding pregnancy.
Her body mass index is 40, and she is normotensive and has a normal serum glucose level. On examination she was tested positive for glucose in urine.
What would be your advice to her?Your Answer: She will be checked for pre-existing diabetes in early pregnancy and, for gestational diabetes at 26 weeks
Explanation:Counselling her about the risks associated with obesity during pregnancy will be the best possible advice to give this patient. A combined follow up by an obstetrician and a diabetes specialist at a high-risk pregnancy clinic is required to formulate the best ways in management of gestation with obesity.
An oral glucose tolerance test should be done at 26 weeks of her pregnancy, along with advising her on controlling her weight by diet and lifestyle modifications. During the early weeks of their pregnancy all obese patients must be routinely tested for pre-existing diabetes.It is highly inappropriate to advice her not to get pregnant.
Without making a proper diagnosis of diabetes, it is wrong to ask her to start oral hypoglycemic agent and/or insulin.
Checking urinary proteins is not indicated at this stage, but can be considered as a part of antenatal check up.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 8
Correct
-
The second meiotic division of the oocyte is normally completed:
Your Answer: After the sperm penetrates the secondary oocyte
Explanation:Upon penetration, if all is normally occurring, the process of egg-activation occurs, and the oocyte is said to have become activated. This is thought to be induced by a specific protein phospholipase c zeta. It undergoes its secondary meiotic division, and the two haploid nuclei (paternal and maternal) fuse to form a zygote.
-
This question is part of the following fields:
- Embryology
-
-
Question 9
Correct
-
You review a 28 year old patient in the fertility clinic. She has a diagnosis of PCOS. She has been trying to conceive for 2 years. Her BMI is 26 kg/m2. She is a non-smoker. She has been taking Clomiphene and metformin for the past 6 months. What is the next most appropriate treatment?
Your Answer: Gonadotrophins
Explanation:Clomiphene shouldn’t be continued for more than 6 months. The second line options are Gonadotrophins or ovarian drilling.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 10
Correct
-
What percentage of pregnancies will be uncomplicated following a single episode of reduced fetal movements?
Your Answer: 70%
Explanation:Reduced fetal movements can be the first indication of possible fetal abnormalities. Movements are first perceived by the mother from about 18-20 weeks gestation, increase in size and frequency until 32 weeks gestation when they plateau at about 31 movements per hour. Investigations for reduced fetal heart rate include auscultation of the fetal heart rate using a handheld doppler device, and a cardiotocograph or ultrasound if the foetus is above 28 weeks gestation. About 70% of women who experience one episode of reduced fetal movement have uncomplicated pregnancies. They are advised to report to a maternal unit if another episode occurs.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 11
Incorrect
-
A 31 year old is being seen in EPU and you are asked to review her ultrasound. There is a solid collection of echoes with numerous small (3-10 mm) anechoic spaces. What is the likely diagnosis?
Your Answer: Partial Molar Pregnancy
Correct Answer: Molar Pregnancy
Explanation:This is typical appearance of molar pregnancy. This used to be referred to as ‘snowstorm sign’ as with older poorer resolution ultrasound the anechoic species looked like a snowstorm.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 12
Incorrect
-
Question 13
Incorrect
-
A 53 year old female presents with hot flushes and night sweats. Her last menstrual period was last year. She had MI recently. Choose the most appropriate management for this patient.
Your Answer: Evening primrose
Correct Answer: Clonidine
Explanation:With a history of MI, oestrogen and COCP should be avoided. Evening primrose is also not suitable for post-menopausal symptoms. Raloxifene is a SERM – these make hot flushes worse. Clonidine will help improve the hot flushes and the vasomotor symptoms.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 14
Correct
-
A women has undergone genetic testing due to her family history and has the BRCA 1 gene. What would you advise her lifetime risk of breast cancer is?
Your Answer: 70%
Explanation:The life time risk of breast cancer in BRCA 1 gene is 70% and of ovarian cancer is 40%.
-
This question is part of the following fields:
- Genetics
-
-
Question 15
Correct
-
Which of the following organisms causes Scarlet Fever?
Your Answer: Streptococcus pyogenes
Explanation:Streptococcus pyogenes, also known as group A beta-haemolytic streptococcus, is the organism responsible for scarlet fever. The bacteria is found in secretions from the nose, ears or the skin, and infections may be preceded by wounds, burns or respiratory infections. Symptoms may include a sore throat, fever, a red skin rash and cervical lymphadenopathy. Untreated scarlet fever in children and adolescents can lead to rheumatic fever, or post-streptococcal glomerulonephritis.
-
This question is part of the following fields:
- Microbiology
-
-
Question 16
Incorrect
-
A 33-year -old G2Pl woman who is at 10 weeks gestation presented to the medical clinic for antenatal visit. It was revealed that she has a twin pregnancy. She was known to have had a complicated previous pregnancy with placental abruption at 34 weeks.
Which of the following is considered the next step in best managing the patient in addition to routine antenatal care?Your Answer: Hospital admission after 34 weeks
Correct Answer: Increased iron and folic acid supplementation
Explanation:Twin pregnancies are at risk for iron deficiency due to significant maternal, fetal, and placental demands. Recommendations regarding the optimal iron dose in twin pregnancies are based on clinical expert opinions, advocating doubling the dose of iron from 30 mg of elemental iron to 60 mg routinely during the second and third trimester, regardless of maternal iron stores.
If pregnant with twins, patient should take the same prenatal vitamins she would take for any pregnancy, but a recommendation of extra folic acid and iron will be made. The additional folic acid and extra iron will help ward off iron-deficiency anaemia, which is more common when patient is pregnant with multiples.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 17
Incorrect
-
A 36 year old woman has a pelvic ultrasound scan showing multiple fibroids. What is the most common form of fibroid degeneration?
Your Answer: Red degeneration
Correct Answer: Hyaline degeneration
Explanation:Hyaline degeneration is the most common form of fibroid degeneration. Fibroids:
Risk Factors
– Black Ethnicity
– Obesity
– Early Puberty
– Increasing age (from puberty until menopause)
Protective Factors
– Pregnancy
– Multiparity -
This question is part of the following fields:
- Clinical Management
-
-
Question 18
Correct
-
A 50-year-old third-generation Australian woman presents with intermittent lower abdominal pain. An abdominal ultrasound was performed and showed a probable malignancy involving the left ovary. The report suggests that the ovarian lesion may represent a metastatic disease.
Which one of the following is the most appropriate investigation that will likely show the site of the primary tumour?Your Answer: Colonoscopy.
Explanation:This woman presents with a metastatic tumour of the ovary. Being from Australia is a hint in this question as the likely site of the primary tumour can vary depending on the country the patient is in and the availability of screening mammography. In underdeveloped countries, breast cancer is usually diagnosed later in life as screening mammography is generally not available, making the most likely site of the primary tumour in the breast. In Japan, where the incidence of stomach cancer is much higher than in western countries, the most likely primary site would be the stomach with a Krukenberg tumour in both ovaries. In Australia, mammographic screening is recommended every other year for all women over the age of 50, and so the most likely primary site would be the colon.
The most appropriate work-up to find the primary tumour in this patient would be performing a colonoscopy. A computed tomography (CT) of the abdomen may miss a small tumour, and an ultrasound examination would not be able to diagnosis a colon cancer. Mammography would be the correct response in under-developed countries. A lung malignancy would be detectable by chest X-ray, but would rarely cause a metastasis in the ovary.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 19
Correct
-
During difficult labour, mediolateral episiotomy is favoured to midline episiotomy because?
Your Answer: Less extension of the incision
Explanation:Mediolateral episiotomy is favoured to midline episiotomy because there is less extension of the incision and decreased chances of injury to the anal sphincter and rectum.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 20
Correct
-
A 34 weeks pregnant patient has a blood pressure of 149/98. Urine dipstick shows protein 3+. You send a for a protein:creatinine ratio. What level would be diagnostic of significant proteinuria?
Your Answer: >30 mg/mmol
Explanation:Pre-eclampsia is defined as hypertension of at least 140/90 mmHg recorded on at least two separate occasions and at least 4 hours apart and in the presence of at least 300 mg protein in a 24 hour collection of urine, arising de novo after the 20th week of pregnancy in a previously normotensive woman and resolving completely by the sixth postpartum week. Significant proteinuria = urinary protein: creatinine ratio >30 mg/mmol or 24-hour urine collection result shows greater than 300 mg protein.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 21
Correct
-
We can detect the fetal heart beat by Sonography (transvaginal) at:
Your Answer: 6 weeks
Explanation:The earliest fetal heart rate detected transvaginally was at 6 weeks 0 days of gestation compared with 7 weeks 0 days transabdominally. The transvaginal Doppler method was also more successful in detecting the fetal heart rate in women with a retroverted uterus (p < or = 0.01).
-
This question is part of the following fields:
- Physiology
-
-
Question 22
Correct
-
Regarding anti-epileptic use in the 1st trimester of pregnancy, which of the following is closely associated with the development of congenital malformations?
Your Answer: Sodium valproate
Explanation:Sodium Valproate is known to be the most teratogenic when used in the first trimester of pregnancy. This antiepileptic increases the risk of congenital malformations including a 10-20 fold risk of neurodevelopmental defects. Though the use of antiepileptics should generally be avoided during pregnancy, carbamazepine, or newer drugs such as Lamotrigine are thought to carry less of a risk of teratogenicity.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 23
Incorrect
-
A 21-year-old nulliparous lady came seeking contraceptive advice. She has never smoked and has no relatives who have been diagnosed with breast cancer or heart disease.
Her weight is 90 kg, her height is 167 cm, her BMI is 32 kg/m2, and her blood pressure is 145/90 mmHg, as recorded on two occasions. She also suffers from hirsutism. she was diagnosed with PCOS.
What are your plans for her?Your Answer: Progestin only pill
Correct Answer: Combined oral contraceptive pill
Explanation:Women with polycystic ovarian syndrome (PCOS) have abnormalities in the metabolism of androgens and oestrogen and in the control of androgen production. PCOS can result from abnormal function of the hypothalamic-pituitary-ovarian (HPO) axis. A woman is diagnosed with polycystic ovaries (as opposed to PCOS) if she has 20 or more follicles in at least 1 ovary. The major features of PCOS include menstrual dysfunction, anovulation, and signs of hyperandrogenism. Other signs and symptoms of PCOS may include the following:
Hirsutism
Infertility
Obesity and metabolic syndrome
Diabetes
Obstructive sleep apnoeaDrugs used in the treatment of polycystic ovarian syndrome (PCOS) include metformin (off-label use), spironolactone, eflornithine (topical cream to treat hirsutism), and oral contraceptives. Oral contraceptives containing a combination of oestrogen and progestin increase sex hormone–binding globulin (SHBG) levels and thereby reduce the free testosterone level. Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) levels are also suppressed. This restores cyclic exposure of the endometrium to oestrogen-progestin, with the resumption of menstrual periods and decreased hirsutism.
Drug of choice for treatment of PCOS are COCs, all other options are incorrect.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 24
Correct
-
A fibroid is a type of
Your Answer: Leiomyoma
Explanation:A fibroid is a benign smooth muscle tumour or Leiomyoma. As such it is something of a misnomer. Leiomyosarcoma and Angioleiomyoma are malignant tumours of smooth muscle under the WHO sort tissue tumour classification Rhabdomyoma is a skeletal muscle tumour Myofibroma is seen in fibromatosis
-
This question is part of the following fields:
- Clinical Management
-
-
Question 25
Incorrect
-
What epithelium cell type lines the ureters?
Your Answer: Columnal
Correct Answer: Transitional
Explanation:Uterus is lines by a single layer of columnar epithelium. The endometrium goes through changes during the menstrual cycles.
-
This question is part of the following fields:
- Pathology
-
-
Question 26
Correct
-
The roof of the femoral triangle is formed by which structure?
Your Answer: Fascia lata
Explanation:The femoral triangle is bounded:
– Superiorly by the inguinal ligament that forms the base of the femoral triangle.
– Medially by the lateral border of the adductor longus.
– Laterally by the sartorius; the apex of the femoral triangle is formed where the borders of the sartorius and the adductor muscles meet.
– The floor of the femoral triangle is formed by the iliopsoas laterally and the pectineus muscle medially.
– The roof of the femoral triangle is formed by the fascia lata and cribriform
fascia, subcutaneous tissue, and skin. -
This question is part of the following fields:
- Anatomy
-
-
Question 27
Incorrect
-
Question 28
Correct
-
The resting pulse in pregnancy is:
Your Answer: Increased by 10 to 15 bpm
Explanation:During pregnancy cardiac output increases by 30 to 50%. As a result, the resting pulse speeds up from a normal of about 70 bpm to 80 or 90 bpm.
-
This question is part of the following fields:
- Physiology
-
-
Question 29
Incorrect
-
Which of the following takes part in the arterial supply of the ovary?
Your Answer: None of the above
Correct Answer: Uterine arteries
Explanation:The ovarian arteries, arising from the abdominal aorta and the ascending uterine arteries which are branches of the internal iliac artery all supply the ovaries. They terminate by bifurcating into the ovarian and tubal branches and anastomose with the contralateral branches providing a collateral circulation.
-
This question is part of the following fields:
- Anatomy
-
-
Question 30
Correct
-
A 34-year-old woman, gravida 1 para 1, presented to the emergency department complaining of left breast pain six weeks after a spontaneous, uncomplicated term vaginal delivery. She reported having noticed the pain and redness on her left breast a week ago. From her unaffected breast, she continued to breastfeed her infant.
Upon history taking, it was noted that she has no chronic medical conditions and for medication, she only takes a daily multivitamin. Her temperature was taken and the result was 38.3 deg C (101 deg F).
Further observation was done and the presence of an erythematous area surrounding a well-circumscribed, 4-cm area of fluctuance extending from the areola to the lateral edge of the left breast was noted. There was also the presence of axillary lymphadenopathy.
Which of the following is the next step to best manage the condition of the patient?Your Answer: Needle aspiration and antibiotics
Explanation:Breast infections can be associated with superficial skin or an underlying lesion. Breast abscesses are more common in lactating women but do occur in nonlactating women as well.
The breast contains breast lobules, each of which drains to a lactiferous duct, which in turn empties to the surface of the nipple. There are lactiferous sinuses which are reservoirs for milk during lactation. The lactiferous ducts undergo epidermalization where keratin production may cause the duct to become obstructed, and in turn, can result in abscess formation. Abscesses associated with lactation usually begin with abrasion or tissue at the nipple, providing an entry point for bacteria. The infection often presents in the second postpartum week and is often precipitated in the presence of milk stasis. The most common organism known to cause a breast abscess is S. aureus, but in some cases, Streptococci, and Staphylococcus epidermidis may also be involved.
The patient will usually provide a history of breast pain, erythema, warmth, and possibly oedema. Patients may provide lactation history. It is important to ask about any history of prior breast infections and the previous treatment. Patients may also complain of fever, nausea, vomiting, purulent drainage from the nipple, or the site of erythema. It is also important to ask about the patient’s medical history, including diabetes. The majority of postpartum mastitis are seen within 6 weeks of while breast-feeding
The patient will have erythema, induration, warmth, and tenderness to palpation at the site in question on the exam. It may feel like there is a palpable mass or area of fluctuance. There may be purulent discharge at the nipple or site of fluctuance. The patient may also have reactive axillary adenopathy. The patient may have a fever or tachycardia on the exam, although these are less common.
Incision and drainage are the standard of care for breast abscesses. If the patient is seen in a primary care setting by a provider that is not comfortable in performing these procedures, the patient may be started on antibiotics and referred to a general surgeon for definitive treatment. Needle aspiration may be attempted for abscesses smaller than 3 cm or in lactational abscesses. A course of antibiotics may be given before or following drainage of breast abscesses.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 31
Correct
-
A 49-year-old lady presents with amenorrhea of 11-months’ duration. Her periods were previously normal and regular. She is planned for an assessment of her FSH (follicle-stimulating hormone) and oestradiol (E2) levels.
Assuming she has attained menopause, which pattern would most likely be found?Your Answer: High FSH and low E2.
Explanation:High FSH and low E2 levels would be expected in menopause. FSH levels would be raised as her body attempts to stimulate ovarian activity and E2 would be low due to reduced ovarian function. The other options would be possible if she was younger, and if occurring with amenorrhea, would warrant further hormonal tests.
It is often challenging to interpret hormone test results close to the time of menopause, especially if the woman is still experiencing irregular menstruation, as remaining ovarian follicles might still produce oestrogen, causing both bleeding and FSH suppression. Elevation of FSH then can be seen again once the oestrogen level drops. Hence, the results would be influenced by the timing of blood sample collection. Once amenorrhea occurs more consistently, it would be easier to interpret the results.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 32
Incorrect
-
You review a 58 year old patient in clinic. She asks what the results of her recent DEXA scan are. You note her hip BMD hip T-score is -1.4. You note she has a history of olecranon fracture 4 years ago. What is her classification according to WHO criteria?
Your Answer: Severe Osteoporosis
Correct Answer: Osteopenia
Explanation:Her T-score puts her in the osteopenic range. The presence of fragility fractures is more important in the osteoporotic patient. Olecranon fracture is not a typical fragility fracture.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 33
Correct
-
An 18 year old and has yet to begin her period. She stands at 4'10. She shows no signs of breast development. She has no pubic hair on pelvic examination. The patient has a cervix and uterus, according to digital inspection. The ovaries cannot be felt. Serum FSH and LH levels are drawn as part of the workup, and both are elevated. Which of the following is the most likely cause of this patient's delayed puberty and sexual infantilism?
Your Answer: Gonadal dysgenesis
Explanation:In girls, delayed puberty and primary amenorrhea may be subdivided according to associated changes in stature. If the affected girl is short, the likely causes are gonadal dysgenesis (Turner syndrome) or hypopituitarism (with both gonadotropin and growth hormone deficiency). Gonadal dysgenesis results from the absence of a sex chromosome or other abnormality of a sex chromosome. In affected girls the gonads are streaks of fibrous tissue and contain no follicles, and these girls may have a variety of congenital anomalies, including a webbed neck, a shieldlike chest, or a small jaw.
Kallmann syndrome presents with amenorrhea, infantile sexual development, low gonadotropins, normal female karyotype, and anosmia (the inability to perceive odours).
In Müllerian agenesis, the Müllerian ducts either fail to develop or regress early in fetal life. These patients have normal ovarian development and normal secondary sexual characteristics. They present with a blind vaginal pouch and no upper vagina, cervix, or uterus, and primary amenorrhea.
The McCune-Albright syndrome rather presents with precocious puberty.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 34
Incorrect
-
Chief role of the mid-cycle LH surge is:
Your Answer: Facilitates oocyte expulsion
Correct Answer: All are correct
Explanation:LH surge occurs around ovulation and it is this LH surge which results in completion of the 1st meiotic division and ovulation occurs. It enhances the production of androgens and also luteinizes the granulosa cells.
-
This question is part of the following fields:
- Physiology
-
-
Question 35
Incorrect
-
The major cause of the increased risk of morbidity & mortality among twin gestation is:
Your Answer: Malpresentation
Correct Answer: Preterm delivery
Explanation:Twin pregnancy is associated with a number of obstetric complications, some of them with serious perinatal consequences, especially for the second twin. The rate of perinatal mortality can be up to six times higher in twin compared to singleton pregnancies, largely due to higher rates of preterm delivery and fetal growth restriction seen in twin pregnancies. Preterm birth and birth weight are also significant determinants of morbidity and mortality into infancy and childhood. More than 50% of twins and almost all triplets are born before 37 weeks of gestation and about 15–20% of admissions to neonatal units are associated with preterm twins and triplets.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 36
Incorrect
-
How many days after fertilisation does the blastocyst hatch from the zone pellucida?
Your Answer: Oct-14
Correct Answer: 5-Jul
Explanation:Shortly after the morula enters the uterus, around the 4th day after fertilization, a clear cystic cavity starts forming inside the morula. The fluid passes through the zona pellucida from the uterine cavity and hence forms the blastocyst.
-
This question is part of the following fields:
- Embryology
-
-
Question 37
Incorrect
-
Which one of the following factors will most likely increase the chances of ovulation in female?
Your Answer: Mittelschmerz
Correct Answer: LH surge
Explanation:Different changes can occur during the menstrual cycle including an increased body temperature at the time of ovulation, thinning of the cervical mucus and few other changes, but it is the LH surge which is the most important factor necessary for ovulation.
Mittelschmerz is characterised by recurrent midcycle pain which occurs around the time of ovulation. -
This question is part of the following fields:
- Physiology
-
-
Question 38
Incorrect
-
A 32-year-old woman, who is 18 weeks pregnant, is diagnosed with antiphospholipid syndrome and positive anticardiolipin antibodies. She has a history of three miscarriages, each one during the first trimester. What would be the next most appropriate step?
Your Answer: Aspirin
Correct Answer: Aspirin & heparin
Explanation:The syndrome with which the woman was diagnosed is an autoimmune, hypercoagulable state which most possibly was the reason of her previous miscarriages. This is the reason why she should be on aspirin and heparin in order to prevent any future miscarriage.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 39
Incorrect
-
A 38-year-old woman presents to the gynaecologic clinic with a complaint of headache, irritability, insomnia, abdominal bloating, anxiety, and breast tenderness around 4 to 5 days before menstruation for the last 8 months. There's also a limitation on daily activities and she has to take a week off from work. The patient's symptoms are relieved with the onset of menstruation. She does not smoke or drink alcohol. There is no other significant past medical history.
Which of the following is the best treatment?Your Answer: Bromocriptine
Correct Answer: Fluoxetine
Explanation:The signs and symptoms of premenstrual dysmorphic disorder are well-known in this patient. Fluoxetine is the greatest therapeutic option among the available options.
For severe symptoms, clomipramine and danazol can be used interchangeably.
Bromocriptine, like oral contraceptives and evening primrose, has no scientific evidence to support its use in this syndrome.
NSAIDs are helpful for painful symptoms, but they only address a limited number of them. -
This question is part of the following fields:
- Gynaecology
-
-
Question 40
Incorrect
-
The most common aetiology for spontaneous abortion of a recognized first trimester gestation:
Your Answer: Maternal hypothyroidism
Correct Answer: Chromosomal anomaly in 50-60% of gestations
Explanation:Chromosomal abnormalities are the most common cause of first trimester miscarriage and are detected in 50-85% of pregnancy tissue specimens after spontaneous miscarriage.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 41
Correct
-
You are asked to assess a patients perineal tear following labour by vaginal delivery. You note a laceration that extends through the vaginal mucosa into the perineal muscle and fascia. The external anal sphincter appears to be in tact. How would you classify this tear?
Your Answer: 2nd
Explanation:If the external anal sphincter is in tact then this is a 1st or 2nd degree tear. As the perineal muscles are involved this is 2nd degree tear.
-
This question is part of the following fields:
- Anatomy
-
-
Question 42
Correct
-
Which of the following contraceptives primary mode of action is inhibition of ovulation?
Your Answer: Cerazette®
Explanation:Traditional POP main mode of contraceptive action: thickening of cervical mucus Desogestrel-only POP main mode of contraceptive action is inhibition of ovulation Cerazette® is the only Desogestrel-only POP in the options above. Other desogestrel brands include: Aizea® Cerelle® Nacrez® The other POPs listed are considered traditional POPs and have the following compositions: Norgeston® – Levonorgestrel 30 mcg Micronor® & Noriday® – Norethisterone 350 mcg Femulen® – Ethynediol diacetate 500 mcg
-
This question is part of the following fields:
- Clinical Management
-
-
Question 43
Correct
-
WHO defines the perinatal mortality rate as
Your Answer: The number of stillbirths and deaths in the first week of life per 1000 births
Explanation:WHO defines perinatal death as the number of still births and death in the first week of life per 1000 births.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 44
Incorrect
-
A 20-year-old female university student, who has never been sexually active, requests advice regarding contraception in view of wanting to start being sexually active.
Which contraceptive option would be most appropriate?Your Answer: The combined oestrogen progestogen contraceptive pill (OCP).
Correct Answer: The OCP and a condom.
Explanation:This patient should be advised to use both an OCP and a condom. The combined oestrogen/progestogen contraceptive pill (COCP) has been found to be very effective. However, she should be made aware that it would not provide any protection from any sexually transmitted diseases so she might still be at risk of developing a STD, depending on her sexual partner preferences. To ensure protection from STDs, she should be advised to use both condoms as well as the combined OCP. An IUCD (intrauterine contraceptive device) would not be preferable if she has multiple sexual partners (high risk of STDs). If she has been screened for STDs, does not actively have an STD and has only one sexual partner then IUCD is a possible option. Some issues that may arise with spermicide use could be related to compliance. This also applies to using condoms alone. These two options are less reliable as compared to COCP.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 45
Incorrect
-
A 32 year old mother is in her first trimester of pregnancy with her second child. She is worried about infections in this pregnancy as her daughter was born with a 'blueberry muffin rash' and was soon found to have sensorineural deafness due to an infection. Which of the following infections is most likely?
Your Answer: Varicella Zoster
Correct Answer: Rubella
Explanation:Congenital infections can be the cause of various congenital abnormalities. Infection with the Rubella virus, part of the TORCH infections (toxoplasmosis, other organisms, rubella, cytomegalovirus, and herpes simplex), can lead to cardiac abnormalities, ophthalmic defects, sensorineural deafness and neurodevelopmental delays. At birth congenital rubella syndrome presents with a petechial rash characteristically dubbed a blueberry muffin rash, and hepatosplenomegaly with jaundice. Immunization of the mother against measles is an effective way of reducing the occurrence of congenital rubella syndrome.
-
This question is part of the following fields:
- Microbiology
-
-
Question 46
Incorrect
-
A 28 year old patient is treated for hydatidiform mole with methotrexate. What is the mechanism of action of methotrexate?
Your Answer: Binds tubulin protein
Correct Answer: Inhibits dihydrofolate reductase
Explanation:Methotrexate is a folic acid antagonist. It inhibits dihydrofolate reductase (DHFR). DHFR catalyses the conversion of dihydrofolate to the active tetrahydrofolate which is required for DNA synthesis. It is either administered as a single intramuscular injection or multiple fixed doses.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 47
Incorrect
-
A patient attends the maternity unit as her waters have broken but she hasn't had contractions. She is 39+6 weeks gestation. Speculum examination confirms prelabour rupture of membranes (PROM). What is the risk of serious neonatal infection with PROM?
Your Answer: 10 in 100
Correct Answer: 1 in 100
Explanation:Prelabour Rupture of Membranes:
– Risk of serious neonatal infection 1% (vs 0.5% for women with intact membranes)
– 60% of patients with PROM will go into labour within 24 hrs
– Induction appropriate if >34 weeks gestation and >24 hours post rupture and patients labour hasn’t started.
– If <34 weeks induction of labour should not be carried out unless there are additional obstetric indications e.g. infection -
This question is part of the following fields:
- Clinical Management
-
-
Question 48
Correct
-
Which of the following regarding the use of tocolytics is true?
Your Answer: Use of a tocolytic drug is not associated with a clear reduction in perinatal or neonatal mortality, or neonatal morbidity
Explanation:Tocolytics are used to suppress contractions. The Canadian preterm labour trial which remains a very influential tocolytic trial to date concluded that tocolytics such as a beta agonist have no significant benefit on perinatal mortality or morbidity or prolong pregnancy to term however it did reduce the number of women delivering within 2 days by 40%. This 48 hour window is the only reason for the use of tocolytics.
Choice of tocolytic (NICE)
1st line: Nifedipine
2nd line: Oxytocin receptor antagonists e.g. atosiban -
This question is part of the following fields:
- Clinical Management
-
-
Question 49
Incorrect
-
You are called to see a 24 year old patient in A&E. She is 34 weeks gestation and her blood pressure is 147/96. Automated reagent strip testing shows protein 2+. You send for a protein:creatinine ratio and this shows a ratio of 36 mg/mmol. What is the appropriate course of action?
Your Answer: Admit and start labetalol
Correct Answer: Admit for observation
Explanation:It is important to be aware of the difference between management of simple hypertension and pre-eclampsia in pregnancy. A BP of 140/90 to 149/99 mmHg is classed as mild hypertension. Without proteinuria this can be monitored once weekly and the patient can be discharged. If proteinuria is present with any degree of hypertension the patient requires admission and BP should be monitored at least 4 times daily according to NICE guidance.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 50
Incorrect
-
A 21-year-old primigravida female presents to the emergency department at 41 weeks gestation.
She complains of a nine hour history of irregular painful contractions.
On examination of her pelvis, her cervix is fully effaced, but only 2 - 3 cm dilated. The fetal head is at the level of the ischial spines in a left occipito-posterior (LOP) position. The membranes ruptured an hour ago.
What would be the best next line of management?Your Answer: Hydration drip of 5% dextrose.
Correct Answer: Oxytocic (Syntocinon4) infusion.
Explanation:The best next line of management is to administer an oxytocic (Syntocinon) infusion.
This is because the progress of labour is slow, and it necessary to augment it. As the membranes have already ruptured, the next step is to increase the contractions and induce labour using an infusion of oxytocic (Syntocinon) infusion.
Extra fluid is also required, but this will be administered alongside the Syntocinon infusion.
A lumbar epidural block is indicated in patients with an occipito-posterior (OP) position. This should not be attempted until more pain relief is required and the progress of labour is reassessed.
A Caesarean section may be necessary due to obstructed labour or fetal distress, it is not indicated at this stage.
Taking blood and holding it in case cross-matching is ultimately required is common, but most patients do not have blood cross-matched prophylactically in case there is a need to be delivered by Caesarean section and require a transfusion.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 51
Incorrect
-
A 39-year-old woman who is 8 weeks pregnant presented to the medical clinic for consultation regarding the chance of her baby having Down syndrome. She mentioned that she has read somewhere that one of the risk factors for Down syndrome is advanced maternal age. She is concerned and asks if there are ways in which she can know whether her baby will be affected.
Which of the following is considered as both the safest and the most accurate diagnostic tool for the exclusion of Down syndrome?Your Answer: Chorionic villus sampling at 10 to 12 weeks of gestation
Correct Answer: Amniocentesis at 16 weeks gestation
Explanation:Amniocentesis is a prenatal procedure performed on a pregnant woman to withdraw a small amount of amniotic fluid from the sac surrounding the foetus.
The goal of amniocentesis is to examine a small amount of this fluid to obtain information about the baby, including its sex, and to detect physical abnormalities such as Down syndrome or spina bifida.
Amniocentesis is only performed on women thought to be at higher risk of delivering a child with a birth defect.Amniocentesis is performed between 16 and 20 weeks into the pregnancy. By around this time, the developing baby is suspended in about 130ml of amniotic fluid, which the baby constantly swallows and excretes. A thin needle is used to withdraw a small amount of this fluid from the sac surrounding the foetus.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 52
Correct
-
A couple in their mid-twenties has chosen the 'Rhythm Strategy' calculation as their contraception method, refraining from sexual activity when a pregnancy might otherwise be possible. They want to avoid having a child for the next two years. For the past twelve months, the lady has kept track of her cycles, which have ranged from 26 to 29 days in duration. Which of the following abstinence durations is the most appropriate?
Your Answer: From day 6 to day 17,
Explanation:To provide suitable advice to this couple, the candidate must be aware of the following facts:
Because the luteal phase is 14 days long, regardless of the follicular phase length, ovulation happens 14 days before the period.
As a result, ovulation in this lady might have occurred as early as day 12 or as late as day 15 of her cycle.
In the presence of adequate and normal cervical mucus, sperm survival has been demonstrated to be far longer than previously thought, with intercourse occurring up to 6 days before the known period of ovulation, resulting in pregnancy.
Intercourse should be stopped six days before the earliest ovulation in this woman (i.e. on day six).
– It is generally accepted that the ovulated egg can be fertilised for approximately 24-36 hours.
Intercourse should not be restarted for at least two days after the most recent ovulation.
This would be day 17 for this woman.
Between days 6 and 17 of the cycle, abstinence is required. -
This question is part of the following fields:
- Gynaecology
-
-
Question 53
Incorrect
-
Regarding menstruation, which of the following is the maximum normal blood loss?
Your Answer: 60-65ml
Correct Answer: 80-85ml
Explanation:Most women lose about 35-40 ml of blood on average during each menstrual cycle. The maximum amount of blood loss is 80 ml after which blood loss of more than 80 ml is defined as heavy menstrual bleeding, formerly known as menorrhagia.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 54
Incorrect
-
You are reviewing a patient with a scan suggestive of partial molar pregnancy. What is the typical genotype of a partial molar pregnancy?
Your Answer: 92 XXXX
Correct Answer: 69 XXY
Explanation:The partial mole is produced when an egg is fertilized by two sperm producing genotype 69 XXY (triploid). It can also occur when one sperm reduplicates itself yielding the genotypes 92 XXXY (tetraploid) though this is less common The genotype of a complete mole is typically 46 XX (diploid) but can also be 46 XY (diploid)
-
This question is part of the following fields:
- Clinical Management
-
-
Question 55
Incorrect
-
A 26-year old woman, 36 weeks age of gestation, is admitted for deep venous thrombosis (DVT) of the right calf. She receives heparin treatment. Which of the following is true regarding the use of heparin rather than a coumarin derivative for anticoagulation?
Your Answer: Rapid metabolism of heparin in the mother minimises placental transfer to the foetus.
Correct Answer: Reversal of the anticoagulant effect of heparin in the mother can be achieved more quickly than that of coumarin, should labour occur.
Explanation:Heparin is a large-sized molecule and does not cross the placenta; it can provide anticoagulation in the mother, however, has no effect on the baby. Heparin is the preferred anticoagulant therapy during pregnancy.
Moreover, the anticoagulant effect of heparin can be rapidly reversed by protamine sulphate.
Warfarin, a coumarin derivative, takes much longer to be reversed compared to heparin. This can be given to the mother between 13 and 36 weeks of pregnancy, however, should be avoided in the first trimester due to its teratogenic effects.
The anticoagulant effect of coumarin derivatives on the baby also takes longer to be reversed. -
This question is part of the following fields:
- Obstetrics
-
-
Question 56
Incorrect
-
Examination of endometrial tissue obtained from a biopsy reveals simple columnar epithelium with no sub-nuclear vacuoles. The stroma is oedematous, & a tortuous gland contains secretions. These findings are consistent with which stage of the menstrual cycle?
Your Answer: Non-ovulatory cycle
Correct Answer: Mid-secretory
Explanation:During mid secretory phase, the endometrium cells undergo distension, become more tortuous and are lined by columnar cells.
In the early proliferative phase, the glandular epithelium is cubo-columnar, while in the late proliferative phase, the glands increase in size, becoming tortuous and there is pseudostratification of the epithelium. -
This question is part of the following fields:
- Physiology
-
-
Question 57
Incorrect
-
All of the following factors increase the risk of endometrial cancer except which one?
Your Answer: PCOS
Correct Answer: High Coffee Consumption
Explanation:The risk factors for uterine carcinoma include obesity, diabetes, Nulliparity, late menopause, unopposed oestrogen therapy, tamoxifen therapy, HRT and a family history of ovarian or uterine carcinoma.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 58
Correct
-
Regarding miscarriage rates, which of the following statements is correct?
Your Answer: In women over 45 years of age miscarriage rate approximately 75%
Explanation:With increasing maternal age, the risk of miscarriage increases. For women between the ages of 40-44, the miscarriage rates sit at about 50% and increases to over 75% for women 45 years and over. The miscarriage rate for women between the ages of 35-39 is 25%.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 59
Incorrect
-
A 37-year-old woman has been taking Microgynon (oral contraceptive pill [OCP]).
When she presents for a repeat prescription, her BP is 160/100 mmHg.
She mentions that she would like to stop the OCP in six months so that she can conceive.
What is the most suitable advice for this woman?Your Answer: Change the OCP to a preparation with a lower oestrogen dose, such as Microgynon 20a.
Correct Answer: Cease the OCP, use condoms for contraception, and reassess the BP in three months.
Explanation:The woman’s blood pressure was elevated at her visit; therefore she should be advised to immediately cease the oral contraceptive pill (OCP) so that the hypertension can resolve without the need for any hypotensive treatment. The blood pressure can then be reassessed in three months. Alternative, non-hormonal birth control methods such as condoms should be used instead.
If her high blood pressure does not resolve, any medication that would be commenced to reduce her blood pressure should be one that is safe to continue when she becomes pregnant.
It is inappropriate to continue the OCP even at a lower dosage or in combination with a hypotensive agent.
Methyldopa has been evaluated and used for treatment of hypertension during pregnancy. There is no clinical evidence to suggest that it causes harm to the foetus or neonate.
Angiotensin converting enzyme (ACE) inhibitors are not approved for use in pregnancy as they have been associated with fetal death in utero. Other antihypertensive agents such as beta-blockers and diuretics are also problematic in pregnancy and should be avoided.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 60
Correct
-
Evidence from a panel of experts is what level of evidence
Your Answer: IV
Explanation:Level I: Evidence obtained from at least one properly designed randomized controlled trial. Level II-1: Evidence obtained from well-designed controlled trials without randomization. Level II-2: Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than one centre or research group. Level II-3: Evidence obtained from multiple time series designs with or without the intervention. Dramatic results in uncontrolled trials might also be regarded as this type of evidence. Level III: Opinions of respected authorities, based on clinical experience, descriptive studies, or reports of expert committees.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 61
Incorrect
-
You are asked to review a patient. They have attended for a scan at 13 weeks following a positive pregnancy test. The patient has had 2 previous pregnancies for which she opted for termination on both occasions. The scan shows no identifiable fetal tissue or gestational sac and you note the radiologist has reported a 'bunch of grapes sign'. What is the likely diagnosis?
Your Answer: Choriocarcinoma
Correct Answer: Complete molar pregnancy
Explanation:Gestational trophoblastic disorder is abnormal conception that is characterised by swollen and oedematous villi with proliferation of the trophoblasts. In a complete mole there is absence of fetal tissue, there is diffuse proliferation of trophoblastic tissue around hydropic villi and on USG it appears as a bunch of grapes or snow storm appearance.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 62
Incorrect
-
All of the following statements regarding human chorionic gonadotrophin are true except::
Your Answer: It is produced by the placenta
Correct Answer: It's level doubles every 48 hours in ectopic pregnancy
Explanation:In normal pregnancy the levels of hCG doubles after every 48-72 hours but in case of ectopic pregnancy the levels of hCG are lower than the normal. It is produced by the placenta and its main role is nourishment of the egg after implantation. Its levels reached a peak at 8-10 weeks of pregnancy and after that the levels decreases for the remainder of pregnancy. In hydatiform mole and trophoblastic diseases its the main hormone for diagnosis of the disease because the levels are highly elevated.
-
This question is part of the following fields:
- Physiology
-
-
Question 63
Incorrect
-
A 31 year old is being seen in EPU and you are asked to review her ultrasound. There is a solid collection of echoes with numerous small (3-10 mm) anechoic spaces. What is the likely diagnosis?
Your Answer: Pregnancy of uncertain viability
Correct Answer: Molar Pregnancy
Explanation:Gestational trophoblastic disorder is characterized by an abnormal trophoblastic proliferation and include a complete and partial mole. It is characterized by persistently elevated BHCG levels after pregnancy and on ultrasound a snow storm appearance. These appear as anechoic areas on ultrasound.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 64
Incorrect
-
A 13-year-old woman is complaining of a lot of acne in her face. Her BMI is 37. She does not have her period yet. She has high insulin levels in her labs. What is the most likely diagnosis?
Your Answer: Acquired hypothyroidism
Correct Answer: Polycystic Ovarian Syndrome (PCOS)
Explanation:The best answer is Polycystic Ovarian Syndrome (PCOS), supported by amenorrhea, obesity and acne. High insulin levels are indicative of PCOS and exclude Cushing syndrome (as this is associated with low insulin levels).
-
This question is part of the following fields:
- Gynaecology
-
-
Question 65
Incorrect
-
A 30 year old woman with a history of two previous C section deliveries, is rushed to the hospital for an emergency c-section at 36 weeks gestation due to antenatal haemorrhage. Upon examination of the uterus, the placenta has invaded the myometrium but the serosa is spared. Which of the following identifies this condition?
Your Answer: Hydatidiform Mole
Correct Answer: Placenta Increta
Explanation:Abnormal placental adherence to the uterus, generally termed Placenta Accreta, is divided into 3 conditions.
– Placenta accreta: refers to the invasion of the chorionic villi beyond the decidual surface of the myometrium.
– Placenta increta: the villi invade deep into the myometrium but spare the serosa;
– Placenta percreta: the chorionic villi invade through the myometrium, penetrate the uterine serosa, and may invade surrounding pelvic structures.These conditions can predispose patients to obstetric bleeding in the third trimester, often requiring emergency intervention.
Risk factors in the development of an abnormal placental adherence include previous c-sections. Placenta Previa, is also a cause of antepartum haemorrhage and serves as a risk factor in the development of abnormal placental adherence.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 66
Incorrect
-
A 32 year old woman with a 6 month history of fatigue and some weight gain reports to clinic for a review. Her medical records show evidence of hypothyroidism. On examination, a non tender, hard goitre is palpated. Further tests reveal elevated anti TPO (anti thyroid peroxidase) and anti -Tg (anti thyroglobulin). Which of the following conditions is most likely to present like this?
Your Answer: Endemic goitres
Correct Answer: Hashimoto's
Explanation:The case presented points to a diagnosis of an autoimmune thyroiditis leading to hypothyroidism. The most common form of autoimmune hypothyroidism, Hashimoto’s, often presents with a goitre, positive for antibody tests against thyroid components i.e. anti-TPO and anti-thyroglobulin. Graves disease and toxic diffuse goitre are more likely to cause hyperthyroidism. While De-Quervain’s and endemic goitre may cause hypothyroidism, they don’t result in positive antibody tests.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 67
Incorrect
-
A 33 year old lady in her first trimester of pregnancy presented with loss of weight, abdominal pain and frequent episodes of vomiting. Her vital signs are normal. She has been given a cyclizine injection but without any significant improvement. The next step would be?
Your Answer: Thiamine
Correct Answer: IV steroids
Explanation:In hyperemesis gravidarum, IV corticosteroids can be given to reduce vomiting, if the patient is not responding to standard anti emetics.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 68
Incorrect
-
In which situation would you prescribe COCs?
Your Answer: A 38 year old woman with history of smoking
Correct Answer: A 20 year old woman with blood pressure 135/80mmHg
Explanation:Absolute contraindications to OCs include breast cancer, history of deep venous thrombosis or pulmonary embolism, active liver disease, use of rifampicin, familial hyperlipidaemia, previous arterial thrombosis, and pregnancy, while relative contraindications include smoking, age over 35, hypertension, breastfeeding, and irregular spontaneous menstruation.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 69
Incorrect
-
Study Z gets funding to increase the population size from 1000 to 2000 patients. What effect is this likely to have on the results?
Your Answer: Increase sensitivity of testing
Correct Answer: Decrease type 2 errors
Explanation:Increasing sample size decreases type 2 errors and increases power of the results. Sensitivity and specificity of the test should remain constant regardless of sample size. Confidence intervals are applied by a statistician and are dependent on the mean.
-
This question is part of the following fields:
- Epidemiology
-
-
Question 70
Incorrect
-
Regarding uterine fibroids, which of the following statements is false?
Your Answer: Approximately 40% of white women had detectable fibroids by 35 years of age
Correct Answer: The risk of fibroids is increased by pregnancy
Explanation:Fibroids are a common gynaecological condition found in many women above the age of 35. They are however uncommon before puberty. They are most common in black women vs white women, and its prevalence increases from puberty to menopause. Risk factors for fibroids include increasing age, obesity and infertility. Protective factors, on the other hand, include pregnancy, as the risk of fibroids decreases with increasing numbers of pregnancies.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 71
Incorrect
-
Which hormone is responsible for contraction of myoepithelial cells in lactation?
Your Answer: Human placental lactogen
Correct Answer: Oxytocin
Explanation:Oxytocin is responsible for the let down mechanism that occurs during breast feeding in which the myothelial cells contract and push the milk into the ductules.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 72
Incorrect
-
A patient is seen in the gynaecology outpatient clinic and is noted to have large volume genital warts perianally and near the urethral meatus. You discuss treatment options and the patient opts for LASER therapy. Which of the following is the most appropriate type of LASER to use?
Your Answer: Diode
Correct Answer: CO2
Explanation:Vulval intraepithelial neoplasia is a premalignant condition which is associated with HPV or lichen sclerosis. Biopsy is essential for diagnosis. Treatment depends of the patients choice and include surgical excision of the area or laser therapy with CO2. Other treatment modalities include immunomodulating creams.
-
This question is part of the following fields:
- Biophysics
-
-
Question 73
Incorrect
-
APGAR's score includes all the following, EXCEPT:
Your Answer: Respirations
Correct Answer: Blood pH
Explanation:Elements of the Apgar score include colour, heart rate, reflexes, muscle tone, and respiration. Apgar scoring is designed to assess for signs of hemodynamic compromise such as cyanosis, hypoperfusion, bradycardia, hypotonia, respiratory depression or apnoea. Each element is scored 0 (zero), 1, or 2. The score is recorded at 1 minute and 5 minutes in all infants with expanded recording at 5-minute intervals for infants who score 7 or less at 5 minutes, and in those requiring resuscitation as a method for monitoring response. Scores of 7 to 10 are considered reassuring.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 74
Incorrect
-
Among the following which will not be elevated in the third trimester of pregnancy?
Your Answer: Serum iron binding capacity
Correct Answer: Serum free T4
Explanation:Normally, there will be a slight raise in prolactin level throughout pregnancy even despite estrogen stimulating and progesterone inhibiting prolactin secretion.
Serum alkaline phosphatase levels will be increased in pregnancy due to placental ALP.
During the first trimester of pregnancy there is a physiological mechanism by hCG causing cross-stimulation of the TSH receptors and as a result of this the concentration of thyroid stimulating hormone (TSH) normally decreases. During second trimester TSH concentration will again return back to its pre-pregnancy levels and then rises slightly by the third trimester. However, most of the changes still occur within the normal non-pregnant range, and the serum free T3 and T4 concentrations remain unchanged throughout pregnancy. But the total concentrations, which include both free and protein-bound fractions, elevates significantly due to an increase in the circulating binding globulins.
Iron binding capacity reflects transferrin, a protein used for iron transportation, which is a globulin found in the beta band on electrophoresis. To counteract the reduction of plasma iron during pregnancy both transferrin and iron binding capacity are elevated during this period.
When compared to the non-pregnant level, cortisol levels are been elevated up to three times than normal.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 75
Incorrect
-
A 26 year old patient who is currently 24 weeks pregnant presents with vaginal discharge. Swabs show Chlamydia Trachomatis detected. Which of the following is the most appropriate treatment regime?
Your Answer: Ofloxacin 400mg once a day for 7 days
Correct Answer: Erythromycin 500 mg twice a day for 14 days
Explanation:The following treatment regimes are recommended for the treatment of Chlamydia in Pregnancy: Erythromycin 500mg four times a day for 7 days or Erythromycin 500 mg twice a day for 14 days or Amoxicillin 500 mg three times a day for 7 days or Azithromycin 1 gm stat (only if no alternative, safety in pregnancy not fully assessed) The following treatment regimes are recommended for the treatment of Chlamydia in NON-PREGNANT patients: Doxycycline 100mg bd for 7 days OR Azithromycin 1gm orally in a single dose NOTE: Doxycycline and Ofloxacin are contraindicated in pregnancy
-
This question is part of the following fields:
- Clinical Management
-
-
Question 76
Correct
-
What is the normal range for variability in cardiotocography (CTG) analysis?
Your Answer: 5-25 bpm
Explanation:Cardiotocography, also known as the non-stress test is used to monitor fetal heartbeat and uterine contractions of the uterus. An abnormal CTG may indicate fetal distress and prompt an early intervention. Variability refers to the variation in the fetal heartbeat form one beat to another. Normal variability is between 5-25 beats per minute while an abnormal variability is less than 5 bpm for more than 50 minutes, or more than 25 bpm for more than 25 minutes.
-
This question is part of the following fields:
- Data Interpretation
-
-
Question 77
Incorrect
-
The following hormones are secreted from the anterior pituitary gland, EXCEPT:
Your Answer: LH
Correct Answer: HCG
Explanation:The following hormones are excreted from the anterior pituitary gland: TSH, GN, ACTH, LH, FSH, MSH, PRL.
Human chorionic gonadotropin (hCG, or human chorionic gonadotrophin) is a placental hormone secreted by syncitiotrophoblasts during the second week of gestation. -
This question is part of the following fields:
- Endocrinology
-
-
Question 78
Incorrect
-
An 20-year-old woman presents to you 6 hours after she was raped on day-12 of her menses which usually lasts for 28 days. You have decided to give her Postinor-2 (levonorgestrel 0.75 mg) as a post-intercourse contraceptive. She is requesting information about any potential adverse effects as well as its efficacy.
Which of the following statements is correct?Your Answer: Menstruation is likely within seven days of the treatment being given.
Correct Answer: The treatment fails to prevent pregnancy in 2-3% of women treated.
Explanation:Postinor-2 (levonorgestrel 750pg) is only an emergency contraceptive and is not designed to be a regular form of contraception. If taken within 24 hours, it is estimated to be able to prevent up 97-98% of pregnancies and 58% if given between 48-72 hours post-unprotected intercourse. It can cause vaginal bleeding within a few days of its administration if it is given before day 8-10 of her menstrual cycle. However, if given mid-cycle, it typically doesn’t affect the timing of her next period unless conception occurs. Nausea and vomiting were common when high doses of OCP were used as a post-intercourse contraceptive. Nausea and vomiting still can occur with Postinor-2, but not up to 50% of women. There is currently no evidence to suggest that the levonorgestrel dose would cause a virilising effect on female foetuses.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 79
Incorrect
-
A patient has had limited response to conservative measures for her overactive bladder (OAB). Which of the following is the most appropriate pharmacological choice?
Your Answer: Imipramine
Correct Answer: Darifenacin
Explanation:Detrusor overactivity can be treated with anti-cholinergic agents such as oxybutynin or tolterodine, solifenacin, fesoterodine and darifenacin. They are used as first line agents. Imipramine is used for enuresis and desmopressin is used for nocturia.
NICE pathwayPrior to initiating anticholinergics:
Bladder training
Consider treating vaginal atrophy and nocturia with topical oestrogen and desmopressin respectively before commencing treatments below.
Consider catheterisation if chronic retention
1st line treatments:
1. Oxybutynin (immediate release) – Do not offer to frail elderly patients
2. Tolterodine (immediate release)
3. Darifenacin (once daily preparation)
DO NOT offer any of the 3 drugs below:
1. Flavoxate
2. Propantheline
3. Imipramine
2nd line treatment
Consider transdermal anticholinergic (antimuscarinic)
Mirabegron
Adjuvant Treatments
Desmopressin can be considered for those with nocturia
Duloxetine may be considered for those who don’t want/unsuitable for surgical treatment
Intravaginal oestrogen can be offered to postmenopausal women with OAB -
This question is part of the following fields:
- Clinical Management
-
-
Question 80
Incorrect
-
A pregnant patient who is needle phobic has her nuchal translucency (NT) scan but refuses serum markers. You advise her the False Positive Rate of the scan is 5%. What would you advise the mother regarding the detection rate of Down Syndrome using NT alone?
Your Answer: 40%
Correct Answer: 70%
Explanation:The nuchal lucency measurement is the measure of the nuchal pad thickness. Children with down syndrome have an increased thickness of the nuchal pad. The risk of down’s syndrome increases with maternal age. The nuchal lucency test has an accuracy rate of 70%.
-
This question is part of the following fields:
- Genetics
-
-
Question 81
Incorrect
-
What is the contraception of choice for epileptics on enzyme inducing antiepileptic drugs?
Your Answer: Progestin -only pills
Correct Answer: Levonorgestrel-releasing intrauterine contraceptive device.
Explanation:Clinical decision making which contraceptive regimen is optimal for an individual woman with epilepsy is one of the most challenging tasks when taking care of women with epilepsy. The bidirectional interactive potential of antiepileptic drugs (AEDs) and hormonal contraceptives needs to be taken into account. Enzyme inducing (EI)-AEDs may reduce the contraceptive efficacy of hormonal contraceptives.
If combined oral contraceptives (COCs) are used in combination with EI-AEDs, it is recommended to choose a COC containing a high progestin dose, well above the dose needed to inhibit ovulation, and to take the COC pill continuously (“long cycle therapy”). But even with the continuous intake of a COC containing a higher progestin dose contraceptive safety cannot be guaranteed, thus additional contraceptive protection may be recommended.
Progestin-only pills (POPs) are likely to be ineffective, if used in combination with EI-AEDs.
Subdermal progestogen implants are not recommended in patients on EI-AEDs, because of published high failure rates.
Depot medroxyprogesterone-acetate (MPA) injections appear to be effective, however they may not be first choice due to serious side effects (delayed return to fertility, impaired bone health).
The use of intrauterine devices is an alternative method of contraception in the majority of women, with the advantage of no relevant drug–drug interactions. The levonorgestrel intrauterine system (IUS) appears to be effective, even in women taking EI-AEDs. Likelihood of serious side effects is low in the IUS users.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 82
Incorrect
-
A couple comes to your clinic because they haven't been able to conceive despite having had frequent sexual activity in the previous 12 months. The female partner is 35 years old and has regular menstrual cycles. The male partner is 38 years old and otherwise normal.
Which of the following studies would you do next to forecast ovulation?Your Answer: Pelvic ultrasound
Correct Answer: Serum progesterone
Explanation:This patient has a regular and long menstrual period. The most crucial thing in this case is to rule out anovulation.
Serum progesterone concentration is the best test for detecting ovulation.
Ovulation has occurred if the level is greater than 20nmol/L.
This test should be performed 3 to 10 days prior to the start of the next anticipated period. -
This question is part of the following fields:
- Gynaecology
-
-
Question 83
Incorrect
-
Question 84
Incorrect
-
A 22-year-old G2P2 who is on her 7th day postpartum called her physician due to her concern of bleeding from the vagina. Upon interview, she described the bleeding to be light pink to bright red and compared with the first few days post-delivery, the bleeding was less heavy. There was also no fever or cramping pain reported by the patient.
Upon examination, it was observed that she is afebrile and her uterus is appropriately sized and non-tender. There was also the presence of about 10cc old, dark blood in her vagina and her cervix was closed.
Which of the following is considered the most appropriate treatment for the patient?Your Answer: Antibiotics for endometritis
Correct Answer: Reassurance
Explanation:The postpartum period begins soon after the baby’s delivery and usually lasts six to eight weeks and ends when the mother’s body has nearly returned to its pre-pregnant state.
Bloody vaginal discharge (lochia rubra) is heavy for the first 3-4 days, and slowly it becomes watery in consistency and colour changes to pinkish-brown (lochia serosa). After the next 10-12 days, it changes to yellowish-white (lochia alba). Advise women to seek medical attention if heavy vaginal bleeding persists (soaking a pad or more in less than an hour). Women with heavy, persistent postpartum bleeding should be evaluated for complications such as retained placenta, uterine atony, rarely invasive placenta, or coagulation disorders. Endometritis may also occur, presenting as fever with no source, maybe accompanied by uterine tenderness and vaginal discharge. This usually requires intravenous antibiotics. This also should be explained and advise the mother to seek immediate medical attention.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 85
Incorrect
-
If your patient is 8 weeks pregnant which one of the following USS measurements is most useful?
Your Answer: Abdominal circumference
Correct Answer: Crown rump length
Explanation:Fetal crown-rump length (CRL) is recommended over last menstrual period for estimating GA when measured in early pregnancy i.e. before 9 to 13+6 weeks.
-
This question is part of the following fields:
- Anatomy
-
-
Question 86
Incorrect
-
A 24 year old female patient undergoes an STI screen due to development of dysuria 5 days earlier. The results are positive for chlamydia infection. With regard to contact tracing what is the recommended action regarding tracing and informing sexual partners in this case?
Your Answer: All sexual partners past 6 weeks
Correct Answer: All sexual partners past 6 months
Explanation:In case a person tests positive for chlamydia, all sexual partners over the period of 6 months should to contacted and started on appropriate antibiotics.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 87
Incorrect
-
Regarding amniotic fluid volume:
Your Answer: Is reduced in severe rhesus disease
Correct Answer: Maybe predicted by ultrasound
Explanation:Amniotic fluid can be measured with the help of ultrasound to gauge the amniotic fluid index. The normal value ranges between 8-18.
Amniocentesis is a procedure by which amniotic fluid is removed. In rhesus disease, it appears yellow due to raised bilirubin levels. -
This question is part of the following fields:
- Physiology
-
-
Question 88
Incorrect
-
In relation to ovulation, when does the LH surge occur?
Your Answer: 1-2 hours before ovulation
Correct Answer: 24-36 hours before ovulation
Explanation:Ovulation usually occurs on day 14 in a typical 28-day cycle. Luteinizing hormone levels spike as a result of increased oestrogen levels secreted from maturing follicles. This LH spike occurs about 24-36 hours before the release of the oocyte from the mature follicle.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 89
Incorrect
-
Which of the following drugs is most associated with coronary artery spasm?
Your Answer: Nifedipine
Correct Answer: Ergometrine
Explanation:Ergot alkaloids e.g. Ergometrine, produce marked and prolonged alpha receptor mediated vasoconstriction. Its overdose can cause ischemia and gangrene of the limbs and bowel. It also causes coronary artery spasm and has been used by cardiologist as a provocation test.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 90
Incorrect
-
The test used to diagnose ovulation on day 21 in a 28 days menstrual cycle is:
Your Answer: Prolactin
Correct Answer: Progesterone
Explanation:After ovulation, the dominant follicle turns into a corpus luteum and begins to secrete progesterone. To confirm ovulation, serum progesterone or its metabolite in urine, can be measured. A single serum progesterone level >3 ng/ml in mid‐luteal phase has been used to retrospectively detect ovulation.
-
This question is part of the following fields:
- Physiology
-
-
Question 91
Correct
-
A pregnant patient with a chest infection is worried about the radiation risk of a chest X Ray. How many days of natural background radiation is equivalent to a chest X Ray?
Your Answer: 2.5
Explanation:X-rays carry low levels of risk during pregnancy and are not a significant cause for concern if the total exposure to ionising radiation is less than 5 rads throughout the pregnancy; a chest X-ray is about 0.00007 rads. The amount of radiation generated from a chest X-ray is equivalent to 2.4 days of natural background radiation. Non-urgent radiological tests should, however, be avoided between 10-17 weeks gestation as there is a higher risk of central nervous system teratogenesis during this time.
-
This question is part of the following fields:
- Biophysics
-
-
Question 92
Incorrect
-
Which of the following drugs is most appropriate to use to stimulate lactation?
Your Answer: Bromocriptine
Correct Answer: Domperidone
Explanation:Domperidone and metoclopramide are D2 dopamine receptor antagonists. They are primarily used to promote gastric motility. They are also known as galactagogues and they promote the production of milk. Cabergoline and bromocriptine are prolactin inhibitors and they reduce milk production.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 93
Incorrect
-
Which one of the following statements regarding oestrogen is correct?
Your Answer: Stimulates sebaceous gland activity
Correct Answer: It is produced in the corpus luteum
Explanation:Oestrogen is secreted by the corpus luteum and is responsible for the proliferation of the endometrium to prepare it for the implantation of the zygote.
-
This question is part of the following fields:
- Physiology
-
-
Question 94
Incorrect
-
Fetal distress commonly occurs when the head is in the occipito-posterior (OP) position during labour. Which of the following statements is the most probable explanation for this?
Your Answer: Obstructed labour.
Correct Answer: Incoordinate uterine action.
Explanation:Incoordinate uterine action almost always results in fetal distress due to increased resting intrauterine pressure. All other statements can also cause fetal distress, however, these are not as common as incoordinate uterine action. Syntocin infusion for labour augmentation and administration of epidural anaesthetic for pain relief can also increase the risk of fetal distress.
Cardiotocograph (CTG) monitoring during labour is highly recommended in patients where the fetal head is found in the OP position. Moreover, it is mandatory when there is Syntocin infusion or epidural anaesthesia. -
This question is part of the following fields:
- Obstetrics
-
-
Question 95
Incorrect
-
The ureters receive autonomic supply from which spinal segments?
Your Answer: T10-12
Correct Answer: T11-L2
Explanation:The ureters receive innervation by a number of nerve plexuses. The nerves supplying the ureters originate from spinal segments T11 to L2. When you think about ureteric colic giving classic ‘loin to groin’ pain it is because the pain is referred to these dermatomes.
-
This question is part of the following fields:
- Anatomy
-
-
Question 96
Incorrect
-
Which of the following best describes the muscles assessed by urodynamic testing?
Your Answer: Detrusor, levator ani and abdominal muscles
Correct Answer: Detrusor and urethral sphincter muscles
Explanation:Urodynamics is a broad term that comprises cytometry, urethral pressure measurement, leak point pressure, pressure flow studies, EMG and videourodynamics. They assess the function of the bladder and urethra as a functional unit. This may provide information such as the site of bladder outlet obstruction, overactivity of the detrusor and sphincter weakness. In muscular terms the detrusor and sphincter muscles are being assessed.
-
This question is part of the following fields:
- Biophysics
-
-
Question 97
Incorrect
-
A 24 week pregnant patient complains of itching over the past 6 weeks particularly to the hands and feet which is worse at night. She has taken cetirizine but this hasn't settled her symptoms. Examination is unremarkable with no rash. What is the likely diagnosis?
Your Answer: Scabies
Correct Answer: Intrahepatic Cholestasis of Pregnancy
Explanation:The history is typical of Intrahepatic Cholestasis of Pregnancy, also known as obstetric cholestasis and prurigo gravidarum. It is characterised by itching without rash and abnormal LFTs beyond normal pregnancy ranges. Itching affects around 23% of pregnancies and can occur before biochemical changes.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 98
Correct
-
A 30-year-old woman in her 36 weeks of gestation, presents for her planned antenatal appointment.
On examination her blood pressure is 150/90 mmHg, in two consecutive readings 5 minutes apart.
Which among the following statements is true regarding gestational hypertension and pre-eclampsia?Your Answer: Pre-eclampsia involves other features in addition to the presence of hypertension
Explanation:Pre-eclampsia presents with other features in addition to the presence of hypertension, also it’s diagnosis cannot be made considered peripheral edema as the only presenting symptom. Proteinuria occurs more commonly in pre-eclampsia than in gestational hypertension and the latter is mostly asymptomatic.
Hypertensive disorders are found to complicate about 10% of all pregnancies. Common one among them is Gestational hypertension, which is defined as the new onset of hypertension after 20 weeks of gestation without any maternal or fetal features of pre-eclampsia, in this case BP will return to normal within three months of postpartum.
Types of hypertensive disorders during pregnancy:
1. Pregnancy-induced hypertension:
a. Systolic blood pressure (SBP) above 140 mm of Hg and diastolic hypertension above 90 mmHg occurring for the first time after the 20th week of pregnancy, which regresses postpartum.
b. The rise in systolic blood pressure above 25 mm of Hg or diastolic blood pressure above 15 mm of Hg from readings before pregnancy or in the first trimester.
2. Mild pre-eclampsia:
BP up to 170/110 mm of Hg in the absence of associated features.
3. Severe pre-eclampsia:
BP above 170/110 mm of Hg and along with features such as kidney impairment, thrombocytopenia, abnormal liver transaminase levels, persistent headache, epigastric tenderness or fetal compromise.
4. Essential (coincidental) hypertension:
Chronic underlying hypertension occurring before the onset of pregnancy or persisting after postpartum.
5. Pregnancy-aggravated hypertension:
Underlying hypertension which is worsened by pregnancy.To diagnose pre-eclampsia clinically, presence of one or more of the following symptoms are required along with a history of onset of hypertension after 20 weeks of gestation.
– Proteinuria: Above 300 mg/24 h or urine protein
reatinine ratio more than 30 mg/mmol.
– Renal insufficiency: serum/plasma creatinine above 0.09 mmol/L or oliguria.
– Liver disease: raised serum transaminases and severe epigastric or right upper quadrant pain.
– Neurological problems: convulsions (eclampsia); hyperreflexia with clonus; severe headaches with hyperreflexia; persistent visual disturbances (scotomata).
– Haematological disturbances like thrombocytopenia; disseminated intravascular coagulation; hemolysis. -
This question is part of the following fields:
- Obstetrics
-
-
Question 99
Incorrect
-
What is the normal maximum endometrial thickness on ultrasound assessment of a post menopausal uterus?
Your Answer: 24mm
Correct Answer: 4mm
Explanation:In post menopausal women the thickness of the endometrium should be 4mm or less or women on tamoxifen is should be less than 5mm. If it is more than this the patient should be worked up for endometrial carcinoma.
-
This question is part of the following fields:
- Biophysics
-
-
Question 100
Incorrect
-
A 27-year-old woman at her 37 weeks of gestation is diagnosed with primary genital herpetic lesions at multiple sites in the genital area.
What is the most appropriate management in this case?Your Answer: Vaginal delivery
Correct Answer: Prophylactic antiviral before 4 days before delivery
Explanation:This woman at her 37 weeks of gestation, has developed multiple herpetic lesions over her genitals. In every case were the mother develops herpes simplex infection after 28 weeks of pregnancy, chances for intrapartum and vertical transmission of the infection to the neonate is considered to be very high.
Risk factors of intrapartum herpes simplex infection of the child includes premature labour, premature rupture of membrane, primary herpes simplex infection and multiple lesion in the genital area.
The most appropriate methods for managing this case includes:
– checking for herpes simplex infection using PCR testing of a cervical swab.
– starting prophylactic antiviral therapy for the mother from 38 weeks of gestation until delivery.
– preferring a cesarean section delivery if there are active lesions present in the cervix and/or vulva.Cesarean delivery is advised in this case along with maternal antiviral therapy before delivery to minimise the risk of vertical transmission.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 101
Incorrect
-
A 28 year old women presents at 30 weeks complaining of intense itching particularly on the hands and feet that is worse in the evenings. She has taken cetirizine but this hasn't settled her symptoms. Examination is unremarkable with no rash. What is the likely diagnosis
Your Answer: Dermatitis artefacta
Correct Answer: Intrahepatic Cholestasis of Pregnancy
Explanation:The history is typical of Intrahepatic Cholestasis of Pregnancy, also known as obstetric cholestasis and prurigo gravidarum. The features are: Intense itching typically of the hands and feet Itch gets worse at night Responds poorly to antihistamines There is no rash. The mechanism is poorly understood but tests may show deranged LFTs. It usually resolves quickly after delivery. The other diagnoses listed are possible though less likely. Scabies normally has a rash
-
This question is part of the following fields:
- Clinical Management
-
-
Question 102
Incorrect
-
A 33-year-old nulliparous pregnant female at the 21st week of pregnancy came to the gynaecological clinic for evaluation of vulval ulcer. A swab was taken revealing the herpes simplex type 2 virus. There is no prior history of such lesions and her partners of the last decade had no history of the infection. She's anxious about how she got the condition and the potential consequences for her and her unborn kid. Which of the following suggestions is the most appropriate?
Your Answer: Treatment with acyclovir will reduce the rate of recurrent disease but is contraindicated in pregnancy because of adverse effects on the foetus.
Correct Answer: The primary infection is commonly asymptomatic.
Explanation:Despite the fact that this question includes many true-false options, the knowledge examined is particularly essential in the treatment of women who have genital herpes.
It answers many of the questions that such women have regarding the disease, how it spreads, how it may be controlled, and how it affects an unborn or recently born child.
All of these issues must be addressed in a counselling question.
Currently, the most prevalent type of genital herpes is type 1, while in the past, type 2 was more common, as confirmed by serology testing.
Type 2 illness is nearly always contracted through sexual contact, but it can go undetected for years.
Acyclovir can be taken during pregnancy, and there are particular reasons for its usage.
Neonatal herpes is most usually diagnosed when the newborn has no cutaneous lesions, and past genital herpes in the mother is protective against neonatal infection, although not always.
Where the genital infection is the initial sign of the disease rather than a relapse of earlier disease, neonatal herpes is far more frequent.
Many patients and doctors are unaware that, while the original infection might be deadly, it is usually asymptomatic.
This explains how the illness spreads between sexual partners when neither has had any previous symptoms of the disease. -
This question is part of the following fields:
- Obstetrics
-
-
Question 103
Incorrect
-
What percentage of children does delayed puberty occur in?
Your Answer: 1%
Correct Answer: 3%
Explanation:Delayed puberty is defined as the absence of breast development in girls beyond the age of 13, and the absence of testicular development in boys beyond the age of 14. The incidence of delayed puberty is 3%, with the condition being more common in boys.
-
This question is part of the following fields:
- Endocrinology
-
-
Question 104
Incorrect
-
A 6-year-old girl is brought to the emergency department for evaluation of vaginal discharge. She has had malodorous vaginal discharge and small amounts of vaginal bleeding for about a week. Her mother called the patient’s primary care provider and instructed to stop giving bubble baths to the child, however, the symptoms have not improved. Aside from the discharge, the girl is normal, she was toilet trained at age 2 and has had no episodes of incontinence. She started kindergarten a month ago. Mother informed that patient has no fever, abdominal pain, or dysuria.
On examination, the labia appear normal but a purulent, malodorous vaginal discharge is noted. Visual inspection with the child in knee-chest position shows a whitish foreign body inside the vaginal introitus.
Which among the following is the best next step in management of this patient?Your Answer: Perform speculum examination under general anesthesia
Correct Answer: Irrigate with warmed fluid after local anesthetic application
Explanation:Vaginal spotting, malodorous vaginal discharge and no signs of trauma like lacerations are the clinical features of vaginal foreign bodies in prepubertal girls. The most common object found as foreign body is toilet paper and its management includes warm irrigation and vaginoscopy under sedation/anesthesia.
Common cause of vulvovaginitis in prepubertal girls are vaginal foreign bodies. Although other objects like small toys, hair bands, etc can be occasionally found, the most common vaginal foreign body is toilet paper. Symptoms like malodorous vaginal discharge, intermittent vaginal bleeding or spotting and urinary symptoms like dysuria are caused due to the chronic irritation caused by the foreign body (the whitish foreign body in this case) on the vaginal tissue.
An external pelvic examination is performed with the girl in a knee-chest or frog-leg position in cases of suspected vaginal foreign body. An attempt at removal, after application of a topical anesthetic in the vaginal introitus, using vaginal irrigation with warm fluid or a swab can be done in case of an easily visualized small foreign body like toilet paper. In cases were the age of the girl or the type of foreign body prohibit adequate clinical evaluation the patient should be sedated or given a general anesthesia for examination using a vaginoscope and the foreign body should be removed.
In cases where child abuse or neglect is suspected Child Protective Services should be contacted. Vaginal or rectal foreign bodies can be the initial presentation of sexual abuse; however in otherwise asymptomatic girls with no behavioral changes, urinary symptoms and vulvar or anal trauma, presence of toilet paper is not of an immediately concerning for abuse.
To evaluate pelvic or ovarian masses CT scan of the abdomen and pelvis can be used; but it is not indicated in evaluation of a vaginal foreign body.
Patients in there prepubertal age have a narrow vaginal introitus and sensitive hymenal tissue due to low estrogen levels, so speculum examinations should not be performed in such patients as it can result in significant discomfort and trauma.
Topical estrogen can be used in the treatment of urethral prolapse, which is a cause of vaginal bleeding in prepubertal girls. This diagnosis is unlikely in this case as those with urethral prolapse will present with a beefy red protrusion at the urethra and not a material in the vagina.
Prepubertal girls with retained toilet paper as a vaginal foreign body will present with symptoms like malodorous vaginal discharge and vaginal spotting secondary to irritation. Initial management is topical anaesthetic application and removal of foreign body either by vaginal irrigation with warm fluid or removal with a swab.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 105
Incorrect
-
Question 106
Correct
-
Which of the following conditions are the most common cause in post-partum haemorrhage?
Your Answer: Uterine atony
Explanation:Uterine atony is the most common cause for postpartum haemorrhage and the conditions like multiple pregnancy, polyhydramnions, macrosomia, prolonged labour and multiparity are the most common risk factor for uterine atony.
Whereas less common causes for postpartum haemorrhage are laceration of genital tract, uterine rupture, uterine inversion and coagulopathy.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 107
Correct
-
In which part of the body does clomiphene trigger ovulation by antagonising oestrogen receptors?
Your Answer: Hypothalamus
Explanation:Clomiphene citrate is widely used in the induction of ovulation, especially in the treatment of anovulatory infertility and in conditions such as PCOS. The drug functions as a selective oestrogen receptor modulator, which acts in the hypothalamus to indicate low serum oestrogen levels. Reduced levels of negative feedback stimulate the secretion of GnRH from the hypothalamus, which in turn stimulate the production of gonadotropins (FSH and LH) from the anterior pituitary. These work to increase ovarian follicular activity.
-
This question is part of the following fields:
- Pharmacology
-
-
Question 108
Incorrect
-
A 24 year old who is 32 weeks pregnant presents with a rash to the abdomen. Looking at the picture below what is the diagnosis?
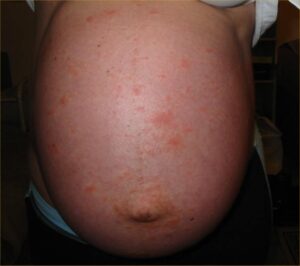
Your Answer: Striae Gravidarum
Correct Answer: Polymorphic Eruption of Pregnancy
Explanation:This is Polymorphic Eruption of Pregnancy (PEP) also known as Pruritic Urticarial Papules and Plaques of Pregnancy (PUPPP). Papules and plaques form on the abdomen (commonly within striae). It is most common in women during their first pregnancy and typically occurs in the 3rd trimester.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 109
Incorrect
-
A 30-year-old pregnant woman, at her 29th week of gestation, presents to physician with flu-like symptoms for the past 3 days along with runny nose, mild headache and she feels achy. She also has mild fever and diffuse rash all over her body. She is concerned about the health of her baby and wants to know if there are any safe medications which will make her feel better in a short time. She has received tetanus vaccination as part of antenatal care program since she immigrated at the end of her first trimester from Romania. Patient is otherwise healthy.
Considering the symptoms and travel history of this patient, she is at higher risk of giving birth to a newborn with which of the following options?Your Answer: Tricuspid valve regurgitation
Correct Answer: Wide pulse pressure
Explanation:This pregnant woman likely has an infection with the rubella virus, which increases the risk of congenital rubella syndrome in her newborn. congenital heart diseases, particularly patent ductus arteriosus (PDA) is a part of this syndrome. Persistence of a patent vessel between the left pulmonary artery and aorta which is supposed to closes in the first 18 hours functionally and in the first 2–3 days of life anatomically is called as PDA.
Normally there is right to left shunting in utero, but in case of PDA blood is shunted from the left (aorta) to the right (pulmonary artery) due to the decrease in pulmonary vascular resistance after birth. This causes right ventricular hypertrophy, if left untreated it can lead to left ventricular hypertrophy and heart failure. There will be a continuous machine-like murmur, heard over the left upper sternal border, as the blood is shunted throughout cardiac cycle. Diastolic BP becomes lower than normal, leading to a higher pulse pressure which is felt as a bounding pulse due to the lost volume from aorta. Though PDA is a non-cyanotic condition, it may lead to Eisenmenger’s syndrome in which R to L shunting persists, resulting in cyanosis, clubbing and polycythemia. Treatment with nonsteroidal anti-inflammatory drugs like indomethacin can close patent PDA. Other symptoms in infants born with rubella syndrome are microcephaly and cataract.
The characteristic feature of an atrial septal defect or ASD, which is a congenital heart disease presenting as an opening in the septa between right and left atria, is a single fixed S2. There will be a delay in closure of the pulmonic valve, due to the excess amount of blood diverted to the right side.
Brachial-femoral delay is a finding in coarctation of aorta, which presents as hypertension in the upper extremities and hypotension in the lower extremities.
A double split S2 is a physiological finding caused by the closure of pulmonary and aortic valves on inspiration.
PDA and pulmonary artery stenosis are the most common cardiac defects reported along with congenital rubella syndrome (CRS), whereas tricuspid valve regurgitation is never reported along with it.
Learning objective: is associated with a continuous machine-like murmur heard over the left upper sternal border, bounding pulse and an increased pulse pressure are the usual symptoms associated with patent ductus arteriosus (PDA), which is mostly seen along with congenital rubella syndrome.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 110
Correct
-
A 27-year-old female reports to the emergency department due to severe right lower quadrant pain. Complaints started yesterday, as the patient noticed intermittent right lower abdominal pain associated with increased activity. She rested for remainder of the day, but the pain still continued to increase. An hour ago, the pain suddenly became constant and severe, associated with nausea and vomiting. The patient does not complaint of any radiation of pain.
On examination patient's temperature is noted to be 37.2 C (99 F), blood pressure is 130/80 mm Hg, and pulse rate is 98/min. On palpation of the right lower quadrant there is tenderness without rebounding or guarding. Urine pregnancy test conducted came to be negative.
Considering the following additional informations, which would be most appropriate in establishing the diagnosis of this patient?Your Answer: History of ovarian cysts
Explanation:Common Risk factors for Ovarian torsion are presence of an ovarian mass, women who are in their reproductive age and history of infertility treatment with ovulation induction.
Common clinical presentations include sudden onset of unilateral pelvic pain along with nausea & vomiting and presence of a palpable adnexal mass. An adnexal mass with absent Doppler flow to ovary can be noted in ultrasound.
Laparoscopy with detorsion, ovarian cystectomy and oophorectomy if necrosis or malignancy is found are the common treatment options.Acute lower abdominal pain in a nonpregnant women can have various causes including pathologies of the gastrointestinal, gynecologic, or urologic systems due to the close proximity of these structures. All of these cases have classic presentations which help to characterize the disease process and thereby to differentiate the diagnosis.
In the given case, patient presents with right lower quadrant pain which is classic for ovarian torsion, occurring due to rotation of the ovary around the infundibulopelvic ligament, causing ovarian vessel occlusion. Although ovarian torsion can occur in any women in their reproductive-age, is seen more commonly in those with a history of ovarian cysts (eg, hemorrhagic cyst) or masses (eg, mature cystic teratoma) because of the greater size and density of the ovary which makes it prone to rotation and subsequent torsion. Patients will initially have intermittent pain associated with activity, as in this patient, due to partial ovarian torsion, this initial pain resolves when the adnexa spontaneously untwists and blood flow returns. When this progresses to complete ovarian torsion, patients typically develop sudden-onset, severe, nonradiating pain due to persistent ischemia, which is often associated with nausea and vomiting.
Ovarian torsion can be clinically diagnosed, but a Doppler ultrasound is performed to evaluate ovarian blood flow and also to confirm the diagnosis. Surgical detorsion to prevent ovarian necrosis and cystectomy/oophorectomy are the usual treatment options.
Any association of urinary symptoms will help to establish a urologic cause of acute right lower quadrant pain like pyelonephritis, nephrolithiasis, etc. However, patients with urologic conditions typically presents with suprapubic or flank pain which radiates to the right lower quadrant, making this diagnosis less likely in the given case.
A family history of malignancy usually does not aid in the diagnosis of acute lower abdominal pain. Although some ovarian cancers are inherited, patients with ovarian cancer typically have a chronic, indolent course with associated weight loss, early satiety, and abdominal distension.
Having multiple sexual partners is considered a risk factor for sexually transmitted infections and pelvic inflammatory disease, which can be a cause for lower abdominal pain. However, patients will typically have fever, constant and diffused pelvic pain along with rebound and guarding.
Recent sick contacts are a risk factor for gastroenteritis, which can present with nausea, vomiting and abdominal pain. However, in this case patient will typically have diffuse, cramping abdominal pain which will worsen gradually; along with persistent vomiting and diarrhea.
Ovarian torsion typically causes intermittent lower abdominal pain followed by sudden-onset of severe, nonradiating unilateral pain with associated nausea and vomiting. Ovarian torsion can occur in women in their reproductive-age, particularly those with a history of ovarian cysts.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 111
Incorrect
-
Branches V2 and V3 of the trigeminal nerve develop from which pharyngeal arch?
Your Answer: 4th
Correct Answer: 1st
Explanation:Trigeminal nerve has three divisions, the first is the ophthalmic division that does not originate from any of the pharyngeal arches, the second and third divisions, namely, the maxillary and the mandibular region develop from the first pharyngeal arch.
Pharyngeal Arches:
1st = Trigeminal V2 & V3 (CN V)
2nd = Facial (CN VII)
3rd = Glossopharyngeal (CN IX)
4th and 6th = Vagus (CN X) -
This question is part of the following fields:
- Embryology
-
-
Question 112
Incorrect
-
The COCP (Combined Oral Contraceptive Pill) causes all of the following biochemical effects EXCEPT which one?
Your Answer: Decreased ovarian androgen synthesis
Correct Answer: Elevate FSH
Explanation:Remember patients with PCOS have elevated LH. COCPs suppress synthesis and secretion of FSH and the mid-cycle surge of LH, thus inhibiting the development of ovarian follicles and ovulation COCPs reduce hyperandrogenism as reduced LH secretion results in decreased ovarian synthesis of androgens. Furthermore they stimulate the liver to produce Sex Hormone Binding Globulin which leads to decreased circulating free androgens. Other mechanisms include reduction in adrenal androgen secretion and inhibition of peripheral conversion of testosterone to dihydrotestosterone and binding of dihydrotestosterone to androgen receptors
-
This question is part of the following fields:
- Clinical Management
-
-
Question 113
Incorrect
-
What is the most common causative organism in Fitzhugh Curtis syndrome and ophthalmic neonatorum?
Your Answer: Toxoplasma Gondii
Correct Answer: Chlamydia trachomatis
Explanation:A rare complication of pelvic inflammatory disease is Fitz Hugh Curtis syndrome which is perihepatitis leading to the formation of adhesions between the liver and the peritoneal surface. It is most commonly caused by chlamydia and gonorrhoea. Ophthalmia neonatorum is conjunctivitis which is also caused by these pathogens.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 114
Incorrect
-
A 30-year-old pregnant woman presents to the emergency department.
She is at 38 weeks gestation and has gone into labour.
On examination, her cervix is 7cm dilated.
Which of the following would be indicative of obstructed labour and the need for delivery by Caesarean section?Your Answer: A maternal fever of 37.8°C.
Correct Answer: A brow presentation in a nulliparous woman.
Explanation:A brow presentation in a nulliparous woman is associated with high risk of obstructed labour and the need for delivery by Caesarean section.
Brow presentation occurs when the presenting part of the fetal head is the part between the orbital ridge and anterior fontanelle.
In multiparous women, the indications differ as vaginal manipulation or spontaneous flexion to a vertex presentation or extension to a face presentation can occur after full cervical dilatation.
Early fetal heart decelerations are indicative of a mild abnormality on cardiotocograph (CTG). It does not indicate obstructive labour or need for delivery by Caesarean section.
The slow descent of the fetal head can be controlled subsequently by good uterine contractions and allow for vaginal birth.
Prolonged labour can cause maternal fever, but that in isolation is not an indication for Caesarean section.
Caput and head moulding are associated with a ‘tight fit’ of the fetal head in the pelvis, but does not contraindicate vaginal birth.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 115
Incorrect
-
A 36-year-old woman is brought to the emergency department after she twisted her ankle, once initial management of her current problem is done, you realize that she is 10 weeks pregnant.
On further questioning, she admits to heroin addiction and says that Doc, I sometimes need to get high on meth, but my favorite wings to fly are cocaine though, since I cannot afford it, I take a bit when I manage to crash a party. She also drinks a bottle of whisky every day. During the past few weeks, she started worrying about not being a good mother, and for this she is taking diazepam at night which she managed to get illegally.
Considering everything this patient revealed, which is most likely to cause fetal malformations?Your Answer: Heroine
Correct Answer: Alcohol
Explanation:Woman in the given case is taking a full bottle of Whisky every day. As per standards, a small glass of Whisky (1.5 Oz) is equivalent of a standard drink and a bottle definitely exceeds 12 standard drinks. This makes her fetus at significant risk for fetal alcohol syndrome (FAS) which is associated with many congenital malformations. Low-set ears, midfacial hypoplasia, elongated philtrum, upturned nose and microcephaly along with skeletal and cardiac malformations are the congenital malformations commonly associated with fetal alcohol syndrome.
Health risks of benzodiazepines during pregnancy has not been clearly established, but there are inconsistent reports of teratogenic effects associated with fetal exposure to benzodiazepines. Neonatal abstinence syndrome of delayed onset can be associated with regular use of benzodiazepine in pregnancy.
Use of Amphetamine in controlled doses during pregnancy is unlikely to pose a substantial teratogenic risk, but a range of obstetric complications such as reduced birth weight and many these outcomes which are not specific to amphetamines but influenced by use of other drug and lifestyle factors in addition to amphetamine are found commonly among women who use it during pregnancy. Exposure to amphetamines in utero may influence prenatal brain development, but the nature of this influence and its potential clinical significance are not well established.
3,4- methylenedioxymetham phetamine(MOMA), which is an amphetamine derivative and commonly known as ecstasy, have existing evidences suggesting that its use during first trimester poses a potential teratogenic risk. So it is strongly recommended to avoided the use of ecstasy during 2-8 weeks post conception or between weeks four to ten after last menstrual period as these are the considered periods of organogenesis.
Role of cocaine in congenital malformations is controversial as cases reported of malformations caused by cocaine are extremely rare. However, it may lead to fetal intracranial haemorrhage leading to a devastating outcome.
Opiate addictions carry a significant risk for several perinatal complications, but it has no proven association with congenital malformation.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 116
Incorrect
-
What type of virus is the Rubella virus?
Your Answer: Double stranded RNA (dsRNA)
Correct Answer: Single stranded RNA (ssRNA)
Explanation:Rubella virus is the only member of the genus Rubivirus and is a type of Togavirus (Togaviridae). It is a single stranded RNA virus. Note for the exam if you are unsure – most RNA viruses encountered in clinical practice are single stranded. The exception is rotavirus which is dsRNA virus. RNA viruses that use DNA during their replication are classed as retroviruses (HIV is an example)
-
This question is part of the following fields:
- Microbiology
-
-
Question 117
Correct
-
Which of the following conditions is associated with blunt trauma in a pregnant woman?
Your Answer: Abruptio placentae
Explanation:Abruptio placentae, defined as a premature separation of the placenta from the uterine wall, is commonly seen with blunt abdominal trauma and can cause fetal distress. It occurs in 1% to 3% of pregnant women with minor trauma and in 40% to 50% with major life-threatening trauma.8,9 Abruption may present with vaginal bleeding, abdominal pain and tenderness, uterine contractions, or fetal distress; however, it may be occult with no vaginal bleeding in up to 20% of cases.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 118
Incorrect
-
A 23-year-old woman at 36 weeks of gestation visits your clinic for follow up.
On pelvic ultrasound you noted a decrease in amniotic fluid, and all her previous scans were normal.
When asked she recollected on experiencing an episode of urinary incontinence yesterday, were she had wet her undergarment with a sudden gush of clear fluid.
Considering the presentation, which of the following is MOST likely the cause of oligohydramnios in this patient?Your Answer:
Correct Answer: Premature preterm rupture of membrane
Explanation:This patient presenting with oligohydramnios in her third trimester and had reported an episode of sudden gush of fluid secondary to ruptured membrane which she had mistaken to be “urinary incontinence”. Hence, the most likely cause of oligohydramnios in this patient will be premature preterm rupture of membrane (PPROM).
An amniotic fluid volume which is less than expected for gestational age is called as Oligohydramnios and is typically diagnosed by ultrasound examination. This condition can be qualitatively described as reduced amniotic fluid volume and quantitatively as amniotic fluid index ≤5 cm or a single deepest pocket <2 cm. Oligohydramnios either can be idiopathic or may have a maternal, fetal or placental cause. Fetal prognosis in this case depends on several factors like the underlying cause, the severity of loss ie. reduced versus no amniotic fluid state and the gestational age at which oligohydramnios occurred. As an adequate volume of amniotic fluid is critical for the normal fetal movements, for fetal lung development and for cushioning the fetus and umbilical cord from uterine compression, so pregnancies complicated with oligohydramnios are at higher risk for fetal deformation, pulmonary hypoplasia and umbilical cord compression.
Oligohydramnios is also associated with an increased risk for fetal or neonatal death, which can either be related to the underlying cause of reduction in amniotic fluid volume or due to the sequelae caused due to reduced amniotic fluid volume. The amniotic fluid volume reflects the balance between fluid production and movement of fluid out of the amniotic sac and the most common mechanisms behind oligohydramnios are fetal oliguria/anuria or fluid loss due to rupture of membranes; also reduction in the amount of lung fluid or increased swallowing do not play major roles in this. Idiopathic cases as in idiopathic oligohydramnios, may be due to alterations in the expression of water pores like aquaporin 1 and aquaporin 3, present in fetal membranes and placenta.Causes of oligohydramnios
a) Maternal causes includes:
– Medical or obstetric conditions associated with uteroplacental insufficiency like preeclampsia, chronic hypertension, collagen vascular disease, nephropathy, thrombophilia.
– Intake of medications like angiotensin converting enzyme inhibitors, prostaglandin synthetase inhibitors, trastuzumab.
b) Placental causes are:
– Abruption of placenta
– Twin polyhydramnios-oligohydramnios sequence which is the Twin to twin transfusion
– Placental thrombosis or infarction
c) Fetal cases leading to oligohydramnios are:
– Chromosomal abnormalities
– Congenital abnormalities which are associated with impaired urine production
– Growth restriction
– Demise
– Post-term pregnancy
– Ruptured fetal membranes
– Infections
– Idiopathic causesDuring First trimester: Etiology of oligohydramnios during the first trimester is often unclear. As the gestational sac fluid is primarily derived from the fetal surface of the placenta via transamniotic flow from the maternal compartment and secretions from the surface of the body of the embryo reduced amniotic fluid prior to 10 weeks of gestation is rare.
During Second trimester: Fetal urine begins to enter the amniotic sac and fetus begins to swallow amniotic fluid by the beginning of second trimester, therefore, during this period any disorders related to the renal/urinary system of the fetus begins to play a prominent role in the etiology of oligohydramnios. Some of such anomalies include intrinsic renal disorders like cystic renal disease and obstructive lesions of the lower urinary tract like posterior urethral valves or urethral atresia. Other common causes of oligohydramnios in the second trimester are maternal and placental factors and traumatic or nontraumatic rupture of the fetal membranes.
During Third trimester: Oligohydramnios which is first diagnosed in the third trimester is often associated with PPROM or with conditions such as preeclampsia or other maternal vascular diseases leading to uteroplacental insufficiency. Oligohydramnios frequently accompanies fetal growth restriction as a result of uteroplacental insufficiency.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 119
Incorrect
-
Due to her inability to conceive, a 28-year-old nulligravid lady comes to the office with her husband. The patient and her spouse had been having intercourse every other day since they stopped using barrier contraception a year ago. Every 28 days, the patient experiences a 5-day period with two days of high flow. She has transient pelvic pain 14 days after her menstruation begins, but intercourse is painless.
The patient was admitted to the hospital in her late teens for a pelvic infection, and she had discomfort with intercourse, discharge, and fever during her stay. She hasn't had any previous medical or surgical procedures. Her younger sibling suffers from polycystic ovarian syndrome. The patient's husband is 32 years old, has no children, and a normal semen analysis. The patient has a blood pressure of 130/80 mm Hg and a pulse rate of 86 beats per minute. There are no anomalies on physical examination.
Which of the following is the most appropriate next step in this patient's care?Your Answer:
Correct Answer: Hysterosalpingogram
Explanation:Primary infertility is defined as the inability to conceive after a year of unprotected, timed sexual intercourse in a nulliparous patient under the age of 35. (After 35 years of age, infertility testing can begin after 6 months.) Because the patient’s partner’s sperm analysis is normal, female factor infertility is the most likely explanation. This patient’s adolescent hospitalizations are likely due to pelvic inflammatory disease (PID), a common cause of infertility caused by tubal scarring and blockage.
A hysterosalpingogram, which includes infusing radiocontrast into the cervix under fluoroscopy, is the first-line imaging technique for determining fallopian tube patency. A hysterosalpingogram is a non-invasive procedure that can detect uterine cavity irregularities (e.g., bicornuate uterus).
Peritoneal adhesions and endometriosis can be seen and treated directly using laparoscopy.
PID-related scarring inside the fallopian tubes can be assessed by laparoscopy with chromotubation; however, it is invasive, expensive, and not utilized first-line.
Ovulation is detected using a mid-cycle LH level. The LH surge can be detected in urine and serum 36 hours before ovulation. Regular menstrual periods are characterized by mittelschmerz (mid-cycle pelvic pain), which indicates ovulation. As a result, an LH level would be useless.
Ovarian reserve begins to deteriorate around the age of 35, and serum FSH levels rise in women who are losing their ability to ovulate. Because this patient is much younger and has regular periods, a drop in ovum quantity is unlikely to be the reason for infertility.
Increased serum androgen levels can prevent ovulation by inhibiting the release of GnRH and FSH through feedback inhibition. The patient has regular cycles and no hyperandrogenic symptoms, despite her sister having polycystic ovarian syndrome (e.g., hirsutism, irregular menses).
In a nulliparous patient under the age of 35, primary infertility is defined as the inability to conceive after a year of unprotected sexual intercourse. A hysterosalpingogram is used to determine the cause of infertility, such as tubal blockage caused by a previous pelvic infection.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 120
Incorrect
-
A 29 year old obese woman presents complaining of difficult or painful sexual intercourse and dysmenorrhea. She is requesting a reversible contraceptive method. Which of the following would be most suitable?
Your Answer:
Correct Answer: Mirena
Explanation:Mirena is a form of contraception also indicated for the treatment of heavy menstrual bleeding and the management of dysmenorrhea, being able to reduce the latter considerably.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 121
Incorrect
-
Regarding missed abortion, all of the following are CORRECT, EXCEPT:
Your Answer:
Correct Answer: Immediate evacuation should be done once the diagnosis is made
Explanation:Expectant management has been reported with unpredictable success rate ranging from 25–76%. Waiting for spontaneous expulsion of the products of conception would waste much time, during which women may suffer uncertainty and anxiety. However, when additional surgical evacuation is needed owing to failure, they may suffer from an emotional breakdown. It is thus not recommended for missed early miscarriage due to the risks of emergency surgical treatment and blood transfusion.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 122
Incorrect
-
You're looking after a 24-year-old woman who is experiencing pelvic pain. She has one-sided pain that is widespread and mild, but can be intense at times. Menstruation has been regular. She denies having fever.
With the exception of a smooth movable adnexal mass on the right side, her pelvic examination seems normal.
Which of the following is the most likely reason for your discomfort?Your Answer:
Correct Answer: Ovarian cyst
Explanation:An ovarian cyst is a sac filled with liquid or semiliquid material that arises in an ovary. Although the discovery of an ovarian cyst causes considerable anxiety in women owing to fears of malignancy, the vast majority of these lesions are benign. Most patients with ovarian cysts are asymptomatic, with the cysts being discovered incidentally during ultrasonography or routine pelvic examination. Some cysts, however, may be associated with a range of symptoms, sometimes severe, including the following:
Pain or discomfort in the lower abdomen
Severe pain from torsion (twisting) or rupture – Cyst rupture is characterized by sudden, sharp, unilateral pelvic pain; this can be associated with trauma, exercise, or coitus. Cyst rupture can lead to peritoneal signs, abdominal distention, and bleeding (which is usually self-limited)
Discomfort with intercourse, particularly deep penetration
Changes in bowel movements such as constipation
Pelvic pressure causing tenesmus or urinary frequency
Menstrual irregularities
Precocious puberty and early menarche in young children
Abdominal fullness and bloating
Indigestion, heartburn, or early satiety
Endometriomas – These are associated with endometriosis, which causes a classic triad of painful and heavy periods and dyspareunia
Tachycardia and hypotension – These may result from haemorrhage caused by cyst rupture
Hyperpyrexia – This may result from some complications of ovarian cysts, such as ovarian torsion
Adnexal or cervical motion tendernessUnderlying malignancy may be associated with early satiety, weight loss
achexia, lymphadenopathy, or shortness of breath related to ascites or pleural effusionThe absence of fever or vaginal discharge rules out PID
The absence of pain on the right lower quadrant, fever, nausea and vomiting rule out appendicitis.
The patient has regular menses, no vaginal bleeding no signs of shock that rules out ectopic pregnancy.
her symptoms are also not consistent with the presentation of leiomyoma. Leiomyoma presents with enlarged uterus, pelvic pressure. It early causes pain when it is complicated with red degeneration which usually occurs in pregnancy.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 123
Incorrect
-
A 26-year-old woman, at 37 weeks and 2 days gestation and currently in her second pregnancy, presents with a breech presentation. She previously delivered a baby girl weighing 3.8kg via spontaneous vaginal delivery at term. Ultrasound examination this time shows a breech presentation with extended legs. She wishes to deliver vaginally if it is possible.
Which is the most appropriate next step to take?
Your Answer:
Correct Answer: Await spontaneous onset of labour.
Explanation:The most suitable step would be to wait for spontaneous onset of labour. This woman would be able to deliver vaginally in 3 situations. The first would be if the foetus is estimated to weigh less than 3800g (first child weight 3800g). Another would be if the foetus is in a frank or complete breech presentation and lastly if the rate of labour progress is satisfactory and breech extraction is unnecessary. RCOG (Royal College of Obstetricians & Gynaecologists) guidelines recommends that women should be informed that elective Caesarean section for the delivery of a breech baby would have a lower risk of perinatal mortality than a planned vaginal delivery. This is because with an elective Caesarean section, we would be able to avoid stillbirth following 39 weeks of gestation as well as intrapartum and vaginal breech delivery risks. The ideal mode of delivery of a breech foetus when labour starts or at least close to term is a Caesarean section as the risks towards the foetus would be significantly increased in a vaginal delivery. The obstetrician is responsible to ensure that there are no other abnormalities that could complicate this even further such as footling presentation, low estimated birth weight (less than 10th centile), hyperextended neck on ultrasound, evidence of fetal distress and high estimated birth weight (>3.8kg). Provided that there is a normal progression of events, fetal risks during both labour and delivery should be low if such factors are absent. Hence, it is right to await the onset of labour to occur spontaneously in this case. In order to exclude a knee presentation with fetal head extension or a footling breech, ultrasound examination has to be done. These are linked to a high fetal risk if the mother attempts vaginal delivery. X-ray pelvimetry is advisable but is not essential in fetal size assessment since its accuracy is roughly 20%. In this case, it is not indicated since there is evidence that her pelvis is of adequate size as she had already delivered a 3.9kg baby prior. It is best to avoid induction of labour in breech cases for numerous reasons (need for augmentation, cord prolapse).
-
This question is part of the following fields:
- Obstetrics
-
-
Question 124
Incorrect
-
Regarding the urinary bladder, what type of epithelium lines it?
Your Answer:
Correct Answer: Transitional
Explanation:The urinary bladder, and most of the urinary structures are lined by epithelium called the urothelium, or the transitional epithelium. This stratified lining is divided into three parts, an apical layer, an intermediate layer and a basal layer. The transitional epithelium is available to stretch to accommodate the increased volume when the bladder is distended, without structural damage.
-
This question is part of the following fields:
- Anatomy
-
-
Question 125
Incorrect
-
A 22-year-old woman who is 28 weeks pregnant presented to the emergency department due to premature uterine contractions. Upon interview, it was noted the she has history of untreated mitral valve stenosis. Tocolysis was then planned after a necessary evaluation was performed and revealed that there is absence of contraindications.
Which of the following would be considered the drug of choice for tocolysis?Your Answer:
Correct Answer: Oxytocin antagonists
Explanation:Tocolysis is an obstetrical procedure to prolong gestation in patients, some of which are experiencing preterm labour. This is achieved through various medications that work to inhibit contractions of uterine smooth muscle.
There is no definitive first-line tocolytic agent by the American College of Obstetrics and Gynecology (ACOG) but nifedipine is most commonly used. However, in severe aortic stenosis, nifedipine can cause ventricular collapse and dysfunction.
The therapeutic target in the treatment of preterm labour is currently the pharmacological inhibition of uterine contractions with the use of various tocolytic agents. Tocolytic agents are used to maintain pregnancy for 24–48 hours to allow corticosteroids administration to act and to permit the transfer of the mother to a centre with a neonatal intensive care unit.
Oxytocin inhibitors work by competitively acting at the oxytocin receptor site. Oxytocin acts to increase the intracellular levels of inositol triphosphate. The medications currently in this class are atosiban and retosiban. Maternal nor fetal side effects have not been described for this tocolytic.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 126
Incorrect
-
A sexually active young woman comes in with frothy, foul-smelling vaginal discharge. Dysuria and dyspareunia are also present. The genital region seems to be quite reddish.
What is the potential danger associated with this presentation?Your Answer:
Correct Answer: Increased risk of cervical cancer
Explanation:TV infection is associated with both LR and HR-HPV infection of the cervix, as well as with ASC-US and HSIL. The signs and symptoms of trichomoniasis are present in this patient. Trichomonas vaginalis is the reason.
Increased vaginal discharge that is frothy, yellowish, and has an unpleasant odour are among the symptoms. It’s frequently linked to dyspareunia and dysuria. Normally, the genital area is red and painful.In both men and women, trichomoniasis can cause preterm labour and raise the risk of infertility. Both the patient and the partner must be treated at the same time.
The active infection can be treated with a single oral dose of metronidazole 2 g taken with food.
To avoid disulfiram-like symptoms, alcohol should be avoided during the first 24-48 hours after treatment. -
This question is part of the following fields:
- Gynaecology
-
-
Question 127
Incorrect
-
A 35-year-old female patient, gravida 1 para 1, visits the clinic to have her contraception method evaluated. The patient has had unpredictable bleeding for the past 8 months since receiving a subdermal progestin implant and begs that it be removed. She used to use combined oral contraceptives and would like to go back to it. The patient has primary hypertension, which she was diagnosed with last year and is effectively controlled on hydrochlorothiazide. She does not take any other medications or have any allergies. Her father and brother both suffer from type 2 diabetes. The patient does not smoke, drink, or use illegal drugs.
24 kg/m2 is her BMI. Blood pressure is 130/75 millimetres of mercury. Physical examinations are all normal. Which of the following is increased by using combination oral contraceptives?Your Answer:
Correct Answer: Worsening hypertension
Explanation:Overt hypertension, developing in about 5% of Pill users, and increases in blood pressure (but within normal limits) in many more is believed to be the result of changes in the renin-angiotensin-aldosterone system, particularly a consistent and marked increase in the plasma renin substrate concentrations. The mechanisms for the hypertensive response are unclear since normal women may demonstrate marked changes in the renin system. A failure of the kidneys to fully suppress renal renin secretion could thus be an important predisposing factor. These observations provide guidelines for the prescription of oral contraceptives. A baseline blood pressure measurement should be obtained, and blood pressure and weight should be followed at 2- or 3-month intervals during treatment. Oral contraceptive therapy should be contraindicated for individuals with a history of hypertension, renal disease, toxaemia, or fluid retention. A positive family history of hypertension, women for whom long-term therapy is indicated, and groups such as blacks, especially prone to hypertensive phenomena, are all relative contraindications for the Pill.
COCs do not increase the risk of developing breast and endometrial cancer, Type 2 DM or breast fibroadenoma.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 128
Incorrect
-
Which of the following is contained within the deep perineal pouch?
Your Answer:
Correct Answer: Proximal portion of urethra
Explanation:The deep perineal pouch contains the external urethral sphincter, proximal urethra in females and membranous urethra in males, deep transverse perineal muscles and the glands of cowper.
-
This question is part of the following fields:
- Anatomy
-
-
Question 129
Incorrect
-
A patients MSU comes back showing heavy growth of E.coli that is resistant to trimethoprim, amoxicillin and nitrofurantoin. You decide to prescribe a course of Cephalexin. What is the mechanism of action of Cephalexin?
Your Answer:
Correct Answer: inhibit peptidoglycan cross-links in bacterial cell wall
Explanation:Cephalosporins are beta lactum drugs, like penicillin. They act by inhibiting the cross linkage of the peptidoglycan wall in bacteria.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 130
Incorrect
-
A 25-year old Asian woman comes to your clinic at 36 weeks of gestation. She was diagnosed with breech at 32 weeks. She is not in labor and a manual examination of the uterus is suggestive of breech position.
Which one of the following would be the next best step in management of this patient?Your Answer:
Correct Answer: Pelvic ultrasound
Explanation:An ultrasonography is performed for confirmation, as well as for the evaluation of maternal pelvis, fetal size and viability in cases were breech presentation is suspected on manual examination. As there is a chance for spontaneous correction of breech presentation into cephalic during 36 to 37 weeks, this should be considered in every future visit. The chances for spontaneous version reduces to 25% if breech position persists beyond this period of time.
It an external cephalic version should be offered to all women with breech presentation, provided there are no contraindications or indication for cesarean delivery due to other reasons.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 131
Incorrect
-
A 25-year-old Aboriginal woman at ten weeks of gestation presents with a 2-week history of nausea, vomiting and dizziness. She has not seen any doctor during this illness.
On examination, she is found to be dehydrated, her heart rate is 135 per minute (sinus tachycardia), blood pressure 96/60 mm of Hg with a postural drop of more than 20 mm of Hg systolic pressure and is unable to tolerate both liquids and solids.Urine contains ketones and blood tests are pending.
How will you manage this case?Your Answer:
Correct Answer: Give metoclopramide and intravenous normal saline
Explanation:Analysis of presentation shows the patient has developed hyperemesis gravidarum.
She is in early shock, presented as sinus tachycardia and hypotension, with ketonuria and requires immediate fluid resuscitation and anti-emetics. The first line fluid of choice is administration of normal saline 0.9%, and should avoid giving dextrose containing fluids as they can precipitate encephalopathy and worsens hyponatremia.The most appropriate management of a pregnant patient in this situation is administration of metoclopramide as the first line and Ondansetron as second line antiemetic, which are Australian category A and B1 drugs respectively. The following also should be considered and monitored for:
1. More refractory vomiting.
2. Failure to improve.
3. Recurrent hospital admissions.Steroids like prednisolone are third line medications which are used in resistant cases of hyperemesis gravidarum after proper consultation.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 132
Incorrect
-
Following parturition uterine contractions called Afterpains may typically continue for how long?
Your Answer:
Correct Answer: 2-3 days
Explanation:Oxytocin can also stimulate after pains that occur 2-3 following delivery.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 133
Incorrect
-
A 28-year-old, 10-weeks pregnant woman comes to you complaining of right iliac fossa pain, which is more when she tries to stand up or cough. She also had a history of appendectomy, done 12 years ago.
Physical examination reveals mild tenderness in right iliac fossa, without any rebound tenderness or guarding.
Among the following options which will be the most likely diagnosis?Your Answer:
Correct Answer: Round ligament pain
Explanation:The given case can be diagnosed as round ligament pain, which is common during pregnancy. This happens as a result to the stretching of round ligament in pelvis to occupy the growing uterus. The round ligament pain usually gets worse with movements or straining and will be relieved by rest or warm application.
As the abdominal examination of patient is unremarkable, conditions like ovarian cyst rupture, ectopic pregnancy and intestinal obstruction are a very unlikely to be the diagnosis.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 134
Incorrect
-
Question 135
Incorrect
-
A 29-year-old nulliparous woman is admitted to the hospital at 37 weeks of gestation after losing about 200 mL of blood per vagina after having sexual intercourse. The bleeding has now ceased and her vitals are below:
Pulse rate: 64 beats/min
Blood pressure: 120/80 mmHg
Temperature: 36.8°C
On physical exam, the uterus is enlarged and is 37 cm above the pubic symphysis. The uterus is lax and non-tender. On ultrasound, the fetal presentation is cephalic with the head freely mobile above the pelvic brim. The fetal heart rate assessed by auscultation is 155 beats/min.
Which of the following is the most likely of bleeding in this patient?Your Answer:
Correct Answer: Placenta praevia.
Explanation:In this pregnant patient with an antepartum haemorrhage at 37 weeks of gestation, her clinical presentation points to a placenta previa. Her bleeding has stopped, the uterus is of the expected size and non-tender, and the fetal head is still mobile above the pelvic brim which are all findings that would be consistent with a placenta praevia. An ultrasound examination would be done to rule-out or diagnose the condition.
An Apt test on the blood is necessary to ensure that this is not fetal blood that would come from a ruptured vasa praevia. Although this diagnosis would be unlikely since the bleeding has stopped. If there was a vasa praevia, there would be fetal tachycardia or bradycardia, where a tachycardia is often seen first but then bradycardia takes over late as fetal exsanguination occurs.
In a placental abruption with concealment of blood loss, the uterus would be larger and some uterine tenderness would be found on exam.
A cervical polyp could bleed after sexual intercourse and a speculum examination would be done to exclude it. However, it would be unlikely for a cervical polyp to cause such a large amount of blood loss. A heavy show would also rarely have as heavy as a loss of 200mL.
-
This question is part of the following fields:
- Obstetrics
-
-
Question 136
Incorrect
-
A 24 year old lady is 9 weeks pregnant with her first child. She attends clinic complaining of severe vomiting and is unable to keep fluids down. The most likely diagnosis is hyperemesis gravidarum. Which of the following is the underlying cause?
Your Answer:
Correct Answer: Increased circulating HCG
Explanation:Hyperemesis gravidarum (HG) is a severe form of nausea and vomiting in pregnancy, associated with weight loss of more than 5% of pre-pregnancy weight, dehydration and electrolyte imbalance. HG is usually most severe during the first 12 weeks of pregnancy and is thought to be caused by high circulating levels of HCG.
There is not yet any evidence that pregnancy itself increases the sensitivity of the area postrema, or that the hormones, oestradiol, or progesterone increase vomiting. Generally, higher concentrations of dopamine stimulates receptors in the chemoreceptor trigger zone leading to nausea and vomiting. Although this has not been demonstrated as the cause of hyperemesis gravidarum.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 137
Incorrect
-
The testicular arteries are branches of what?
Your Answer:
Correct Answer: Aorta
Explanation:The testicular artery arises from the aorta and supplies the testis and the epididymis. The testis is supplied by 3 arteries.: Testicular artery, cremasteric artery that arises from the inferior hypogastric artery and the artery to the vas deferens from the internal iliac artery.
-
This question is part of the following fields:
- Anatomy
-
-
Question 138
Incorrect
-
At ovulation the surge in LH causes rupture of the mature oocyte via action on what?
Your Answer:
Correct Answer: Theca externa
Explanation:The luteinizing hormone (LH) surge during ovulation causes: Increases cAMP resulting in increased progesterone and PGF2 production PGF2 causes contraction of theca externa smooth muscle cells resulting in rupture of the mature oocyte
-
This question is part of the following fields:
- Endocrinology
-
-
Question 139
Incorrect
-
A patient undergoes oophorectomy and the ovarian veins are ligated. Which vein does the right ovary drain into?
Your Answer:
Correct Answer: Inferior vena cava
Explanation:The right ovarian vein travels through the suspensory ligament of the ovary and generally joins the inferior vena cava whereas the left ovarian vein drains into the left renal vein.
-
This question is part of the following fields:
- Anatomy
-
-
Question 140
Incorrect
-
A 46 year old women with a BMI of 34 is seen in clinic following hysteroscopy and biopsy for irregular menstrual bleeding. Histology shows atypical hyperplasia. Which of the following is the most appropriate 1st line management?
Your Answer:
Correct Answer: Laparoscopic hysterectomy
Explanation:There is an increase risk of developing carcinoma of the uterus, if the endometrium shows hyperplasia with atypia. The standard surgery is total hysterectomy with bilateral salpingectomy which can be performed abdominally or laparoscopically If the disease is grade 1-2 and less than 1B i.e. less than 50% invasion of the uterine body.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 141
Incorrect
-
Which of the following is regarded as the current Gold standard in the diagnosis of Polycystic Ovary Syndrome?
Your Answer:
Correct Answer: Rotterdam
Explanation:The Rotterdam criteria was developed and expanded by the European Society of Human Reproduction and Embryology/American Society for Reproductive Medicine Rotterdam consensus (ESHRE/ASRM) in 2003 and is now the Gold standard in the diagnosis of PCOS. The criteria requires two of three features: anovulation, hyperandrogenism, and polycystic ovaries seen on ultrasound.
The National Institute of Child Health and Human Development (NICHD) attempted to define PCOS in 1990 but omitted ultrasonographic evidence of polycystic ovaries which is considered to be diagnostic of PCOS.
The Androgen Excess Society (AES) served to confirm hyperandrogenism as the central event in the development of PCOS.
The ROME III criteria is used for Irritable Bowel Disease and is therefore not applicable to PCOS.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 142
Incorrect
-
You see a patient on the ward who is acutely short of breath and perform an ABG. The results are as follows
Your Answer:
Correct Answer: Respiratory Acidosis
Explanation:This patient has acidosis as the pH is low <7.35 The pO2 is irrelevant. The pCO2 is raised i.e. the respiratory system is causing acidosis. The patient is acidotic so this is a respiratory acidosis The Base Excess is normal. You would typically expect the base excess to rise but metabolic compensation is slower than respiratory compensation so this picture may be seen acutely.
-
This question is part of the following fields:
- Biochemistry
-
-
Question 143
Incorrect
-
Which of the following inhibit Glucagon?
Your Answer:
Correct Answer: Uraemia
Explanation:Glucagon release is inhibited by increased blood glucose, ketones, free fatty
acids, insulin, raised urea levels and somatostatin. Glucagon is produced by alpha cells of the pancreas and increases the plasma glucose level by stimulating glycogenolysis and gluconeogenesis. -
This question is part of the following fields:
- Endocrinology
-
-
Question 144
Incorrect
-
You diagnose Erb-Duchenne palsy in a baby born with shoulder dystocia who suffered a brachial plexus injury. Which of the following nerve roots are likely to be affected?
Your Answer:
Correct Answer: C5 and C6
Explanation:Shoulder dystocia occurs when the fetal shoulder impacts on the maternal symphysis or sacrum during vaginal delivery. About 10% of babies with shoulder dystocia will suffer a brachial plexus injury, the most common one being Erb-Duchenne palsy. In Erb’s palsy, the upper nerve roots C5 and C6 are damaged due to excessive widening of the angle between the head and the shoulder. This causing temporary paralysis in the affected arm whereby the infant will present with its hand hanging limp by his side, internal rotation of the forearm, plus wrist and finger flexion. This sign is called the ‘waiter’s tip hand’. The palsy usually resolves spontaneously in a large proportion of cases.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 145
Incorrect
-
Bladder neck closure and relaxation of the bladder is mediated by?
Your Answer:
Correct Answer: Sympathetic Fibres L1,L2
Explanation:The neck of the bladder is surrounded by the internal sphincter. It is supplied by the sympathetic and parasympathetic nerves of the splanchnic nerve. Parasympathetic stimulation causes the detrusor muscle to contract and the internal urethral sphincter to relax. It Is predominantly by the parasympathetic nerves S2-S4. Relaxation of the bladder is caused by inhibiting the sacral parasympathetic preganglionic neurons and exciting the lumbar sympathetic preganglionic neurons. Remember SYMPATHETIC is for STORAGE and PARASYMPATHETIC is for PEEING.
-
This question is part of the following fields:
- Anatomy
-
-
Question 146
Incorrect
-
A 30-year-old woman presents to the clinic.
She complains of a 6 week history of amenorrhoea and on diagnostic testing, has a positive pregnancy test.
On past medical history, it is noted that she had a multiload (Cu375°) intrauterine device inserted six months ago.
On physical examination, The strings of the device are not visibly protruding through the external os, as would be expected.
She is happy to proceed with the pregnancy, and asks what should be done next.
What is the best next step in her management?Your Answer:
Correct Answer: Ultrasound of the pelvis.
Explanation:The best next step is to order an ultrasound of the pelvis to locate the IUCD in the uterine cavity.
Once the device is located, appropriate advice can be given about the pregnancy proceeding.
Uterine sounding and hysteroscopy are contraindicated in the presence of a viable pregnancy due to risks of infection and abortion.
Pelvic X-ray is indicated if the device cannot be located during the pelvic ultrasound. It can show if the device is in the peritoneal cavity or has been expelled from the uterus. It should only be done after the pregnancy.
In cases where the device is in the peritoneal cavity, a laparoscopy is indicated for device removal.
Pregnancy termination is not indicated simply because of the presence of an intrauterine device (IUCD) in the uterus, unless other factors dictate that this is appropriate.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 147
Incorrect
-
What is the male infertility rate in CF patients?
Your Answer:
Correct Answer: 98%
Explanation:Cystic fibrosis is the most common fetal genetic disease in Caucasians and has an autosomal recessive inheritance. It is caused by an abnormal chloride channel due to a defect in the CFTR gene. Complications range from haemoptysis, respiratory failure, biliary cirrhosis, diabetes and male infertility. Men with CF are infertile in 98% of the cases due to failure of development of the vas deference.
-
This question is part of the following fields:
- Clinical Management
-
-
Question 148
Incorrect
-
A 38-year-old female patient comes to your office complaining of a foul-smelling grey vaginal discharge. Bacteria adhering to vaginal epithelial cells are visible under light microscopy using a wet mount preparation.
Which of the following creatures is most likely to be a pathogen?Your Answer:
Correct Answer: Gardnerella vaginalis
Explanation:Gardnerella vaginalis is one of the bacteria implicated in the development of bacterial vaginosis , many women (>50%) with this vaginal infection have no signs or symptoms, when these are present they are most often :
Vaginal discharge, grey, white or green, with a strong unpleasant odour
Strong vaginal odour and fishy smell after sex
Vaginal itching
Burning during urination
Vaginal bleeding after sex
Gardnerella vaginalis can also be responsible for serious infections (sepsis, wound infections) in locations other than those associated with the genital tract or obstetrics, these cases are very rare but have been reported, including in men.Mycoplasma Hominis is one of the organisms involved in the pathogenesis of BV but it appears normal on wet mount.
Candida presents with white cottage cheese like discharge.
Chlamydia is not seen on wet mount and produces clear vaginal discharge.
Trichomonas shows clue cells on wet mount.
-
This question is part of the following fields:
- Gynaecology
-
-
Question 149
Incorrect
-
The pelvis includes which of the following bones:
Your Answer:
Correct Answer: Ilium, ischium, pubis, sacrum & coccyx
Explanation:The pelvic skeleton is formed posteriorly (in the area of the back), by the sacrum and the coccyx and laterally and anteriorly (forward and to the sides), by a pair of hip bones. Each hip bone consists of 3 sections, ilium, ischium, and pubis.
-
This question is part of the following fields:
- Anatomy
-
-
Question 150
Incorrect
-
Which HPV subtypes are chiefly associated with causing cancer?
Your Answer:
Correct Answer: 16 and 18
Explanation:HPV 16 and 18 are responsible for 70% of cases of HPV related cancers. They are considered the most important high risk genotypes of HPV. As well as cervical cancer they are associated with cancers of the oropharynx and anogenital region.
There are over 100 genotypes of HPV including several other high risk HPV types. Gardasil® is a quadrivalent vaccine against HPV Types 6, 11, 16, and 18
HPV genotypes 6 and 11 are low risk and cause anogenital warts.
Typically 70% of HPV infections are cleared within 1 year and 90% are cleared within 2 years
-
This question is part of the following fields:
- Microbiology
-
00
Correct
00
Incorrect
00
:
00
:
0
00
Session Time
00
:
00
Average Question Time (
Mins)